

Indications
1. Detection of stenosis or occlusions in segments of the peripheral arteries.
2. Monitoring of sites of previous surgical interventions, including sites of previous bypass.
3. Monitoring of sites of various percutaneous interventions.
4. Follow-up of previously diagnosed disease.
5. Evaluation of arterial integrity in the setting of trauma.
Anatomy
Having a well rounded working knowledge of the arterial anatomy helps immensely when performing these exams. Let’s begin with the upper system.
The aorta is the main artery of the body arising from the outflow tract of the left ventricle. It is shaped like an umbrella handle or a candy cane. The first portion is the ascending aorta which then curves to become the aortic arch. Here there are three consecutive vessels that arise and course cephalad. The first is the brachiocephalic or innonimate artery which further bifurcates into right subclavian and common carotid arteries. Next is the left common carotid artery followed immediately by the left subclavian artery.
Lower Extremity
After the three aortic arch vessels the aorta dips down and becomes the descending thoracic aorta. Once it pierces the diaphragm it transforms into the abdominal aorta.
The aorta continues to travel down giving off branches to the intestines and abdominal viscera finally terminating in a bifurcation. These two vessels are known as the common iliac arteries.


The iliac arteries bifurcate into external and internal iliac arteries (EIA and IIA). The EIA continues caudally turning into the common femoral artery (CFA) which further bifurcates into superficial femoral (SFA) and deep femoral artery (aka profunda femoris). The SFA then converts into the popliteal artery which bifurcates into the tibioperoneal trunk and anterior tibial artery (ATA). The tibioperoneal trunk bifurcates into posterior tibial artery (PTA) and the peroneal artery. The anterior tibial artery descends further to become the dorsalis pedis artery (DPA).

Common Iliac and its branches 
External Iliac Artery 
Common Femoral Artery 
CFA and its branches 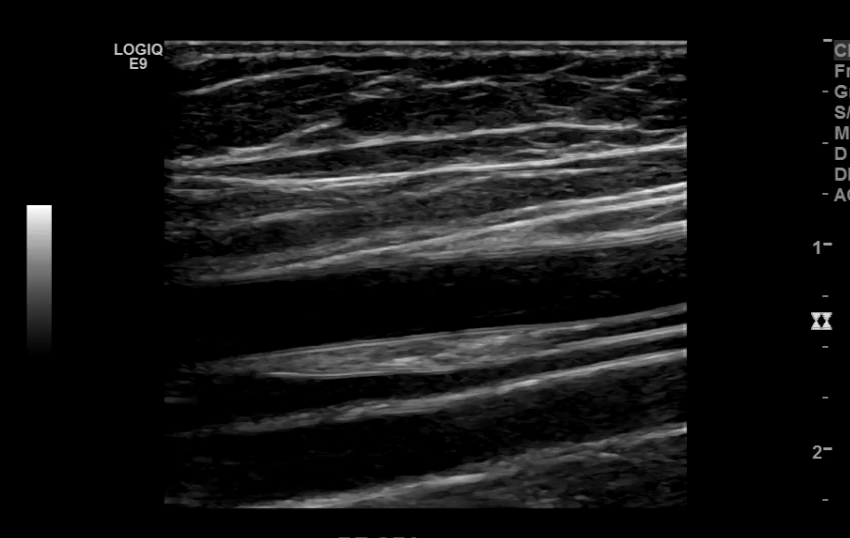
Superficial Femoral Artery 
Popliteal Artery 
Tibioperoneal Trunk 
Posterior Tibial Artery 
Anterior Tibial Artery 
Dorsalis Pedis Artery

Technique
Taking technically superior images not only looks aesthetically pleasing, it is important in that it provides accurate data to render a correct diagnosis. A few parameters you may want to tweak are the doppler scale or pulse repetition frequency PRF and gain for both color and spectral doppler.
Too low of a scale and you’ll get aliasing which makes getting a proper velocity impossible.

Scale/PRF too low 
Scale/PRF too high 
Gain too high 
Gain too low 
Optimal Doppler settings
Other parameters to consider are sweep speed, wall filters, color box size and orientation, sample box size and whether you’re color scale is inverted to name a few.

TGC’s not optimized 
TGC’s optimized

Aliasing from low PRF 
PRF too high 
PRF optimized

Sweep Speed set at zero 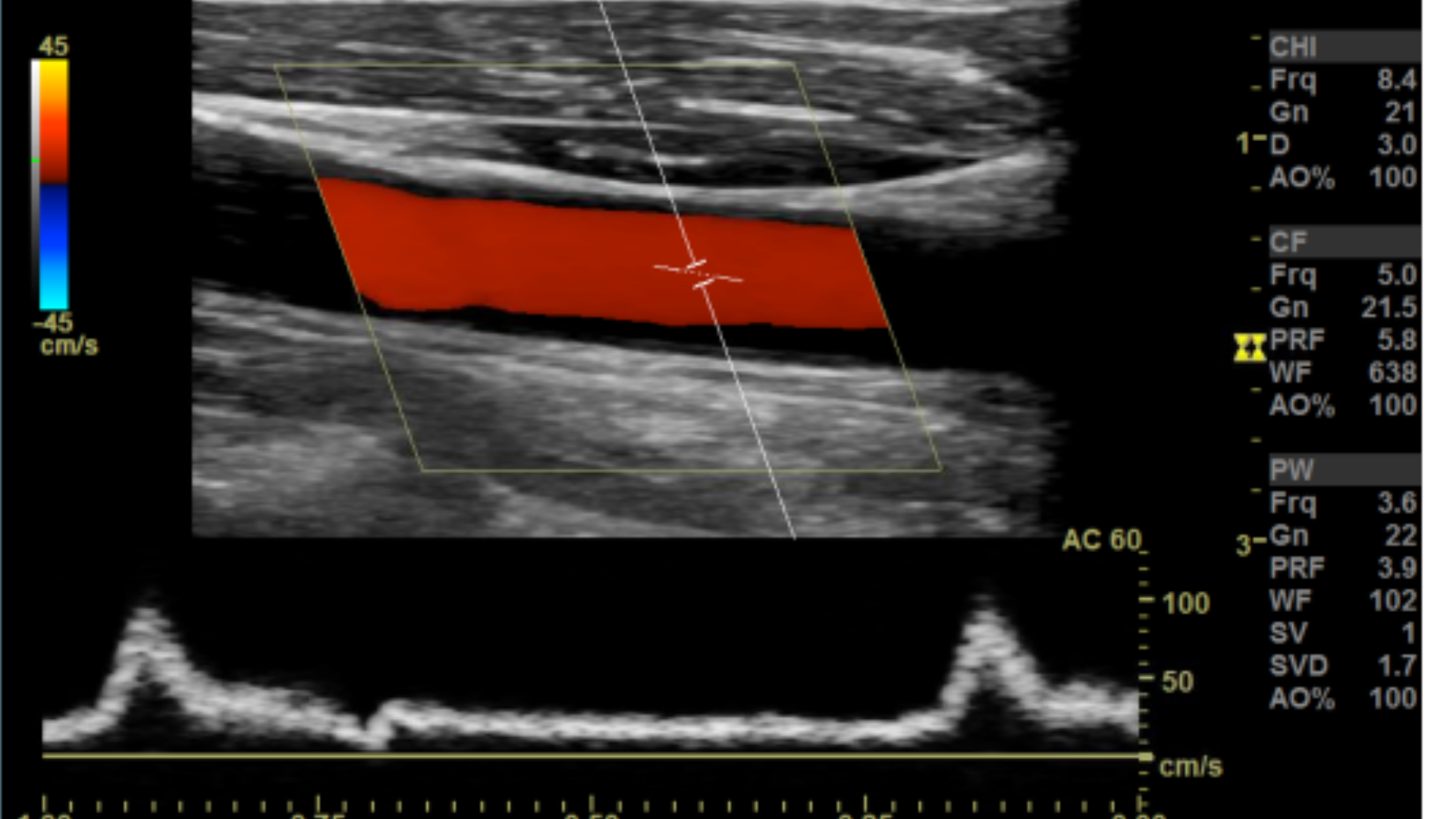
Sweep speed set at 7 
Sweep Speed set at 4
Many people have trouble on how to set the color box. A quick way to get it right is to make sure the steered ultrasound beam and vessel meet an acute angle 60° or less.


Correct Color box angle 
Sub-optimal angle 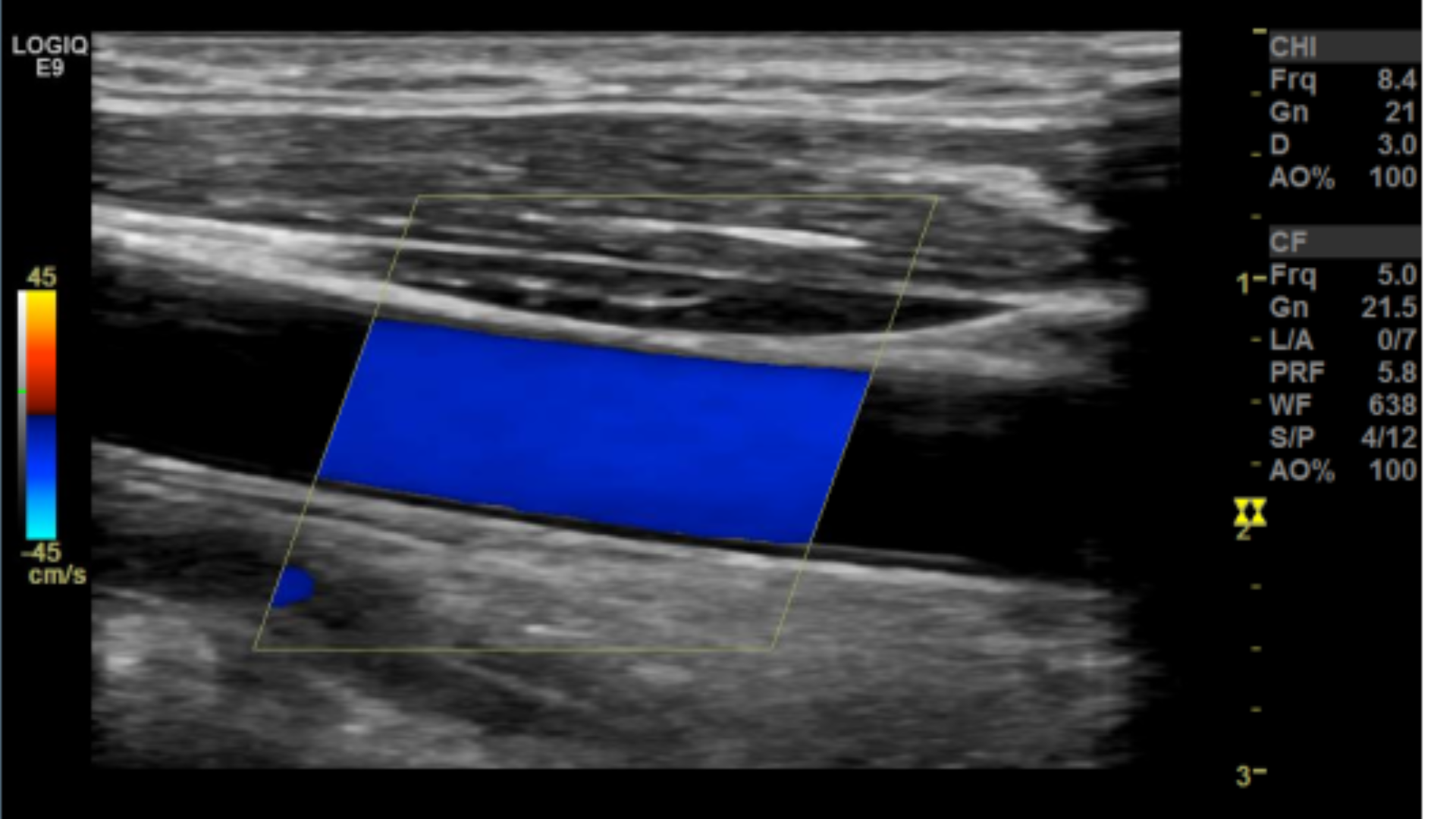
Incorrect angle
Protocol
Lower Extremity Duplex

Great- thank you
LikeLiked by 1 person
You bet
LikeLike
Question: When doing UE arterial’s our muscle memory can work against us depending on how the arm is resting (being sagittal could mean your transducer notch is facing away from you) Would you EVER consider holding the transducer in a more comfortable position (+muscle memory) by holding it such that the notch of transducer is “wrong” ie facing the patient’s hand? I admit to doing this and no rad has ever said anything, however I know it goes against convention.
LikeLike
In sagittal the transducer should face the patients head, and in transverse it should face the patients right
LikeLike
VERY USEFUL. SIMPLIFIED
LikeLike