

According to the CDC Stroke is the 5th leading cause of death (133,103) [1]
Carotid examination is the initial exam in evaluating atherlosclerotic disease. In this video I am going to cover the anatomy of the extracranial arteries, go over the protocol of duplex examination and briefly cover pathology at the end.
Indications
Syncope
Stroke
AMS
TIA
Bruit
Follow up known stenosis
Anatomy
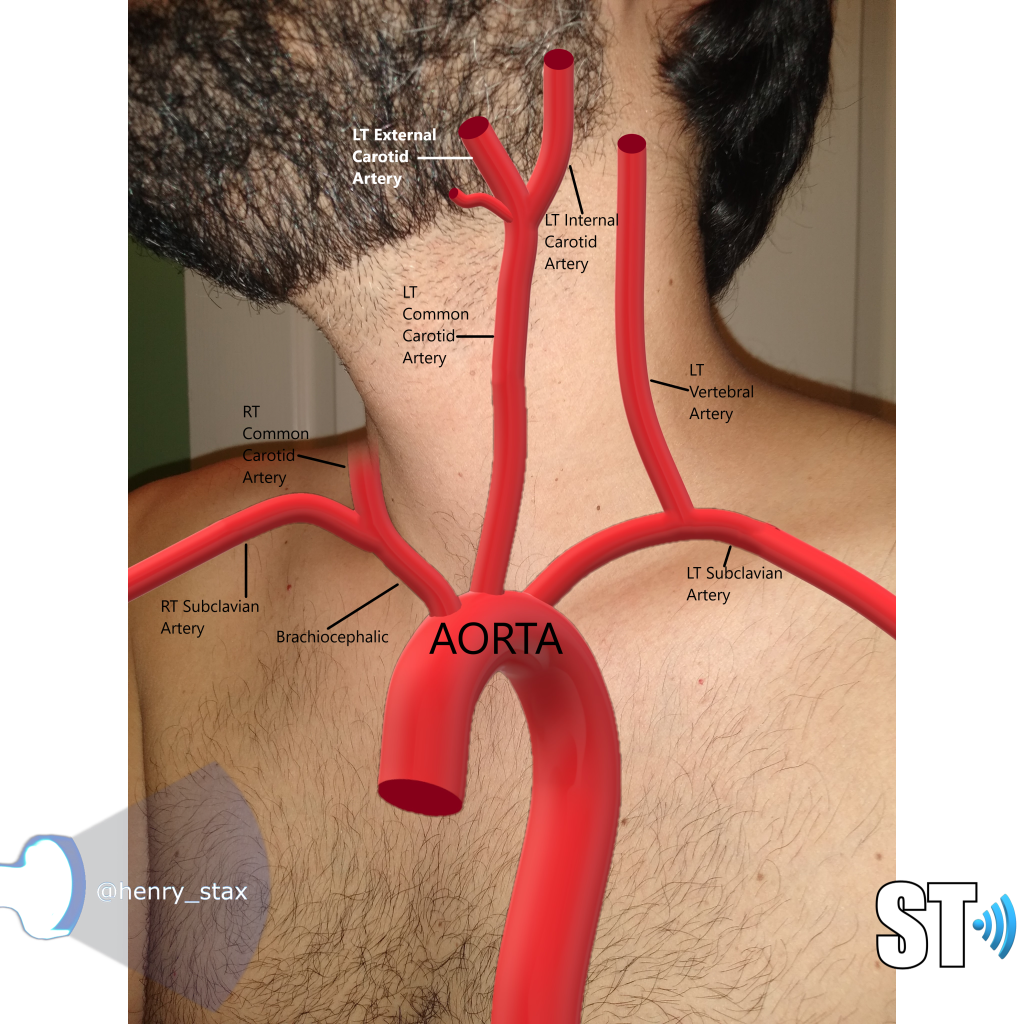
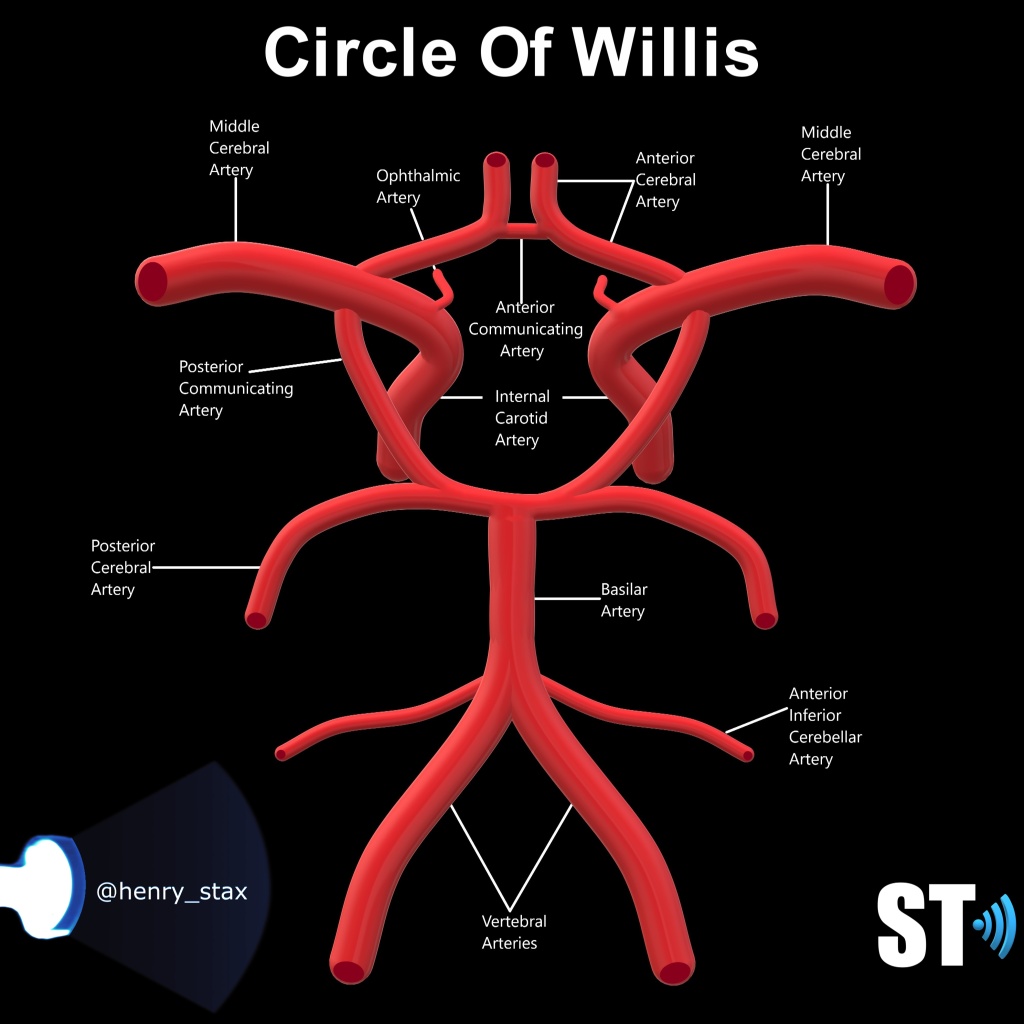
The brain is fed oxygenated blood by paired vessels that arises from the aortic arch. The typical configuration consists of 3 vessels; the RT brachiocephalic also called the innonimate, which in turn bifurcates into the Rt subclavian and common carotid artery, The left common carotid artery (CCA) and the LT subclavian artery (SCLVA). There are variations to this anatomy, though 73% of the population has this configuration. [2] The common carotid arteries further bifurcate into the internal and external carotid arteries at the carotid bulb, which feed the brain (ICA) and face/neck (ECA) respectively. The vertebral arteries (VA) arise from the SCLVA and traverse cephalad through the transverse foramina of the cervical vertebrae c1-c6, entering the brain through the posterior fossa. [3] The confluence of all these vessels join to make the circle of Willis, a circular anastomotic arterial network at the base of the brain.
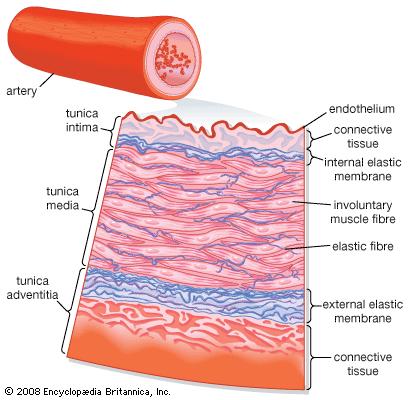
The walls of an artery, much like the veins consist of 3 layers, the Tunica interna, media and adventia. (Inner, middle, and outer layers), the difference being the middle muscular layer of arteries are thicker. This is important to know because this is where plaque builds up.
Flow Characteristics
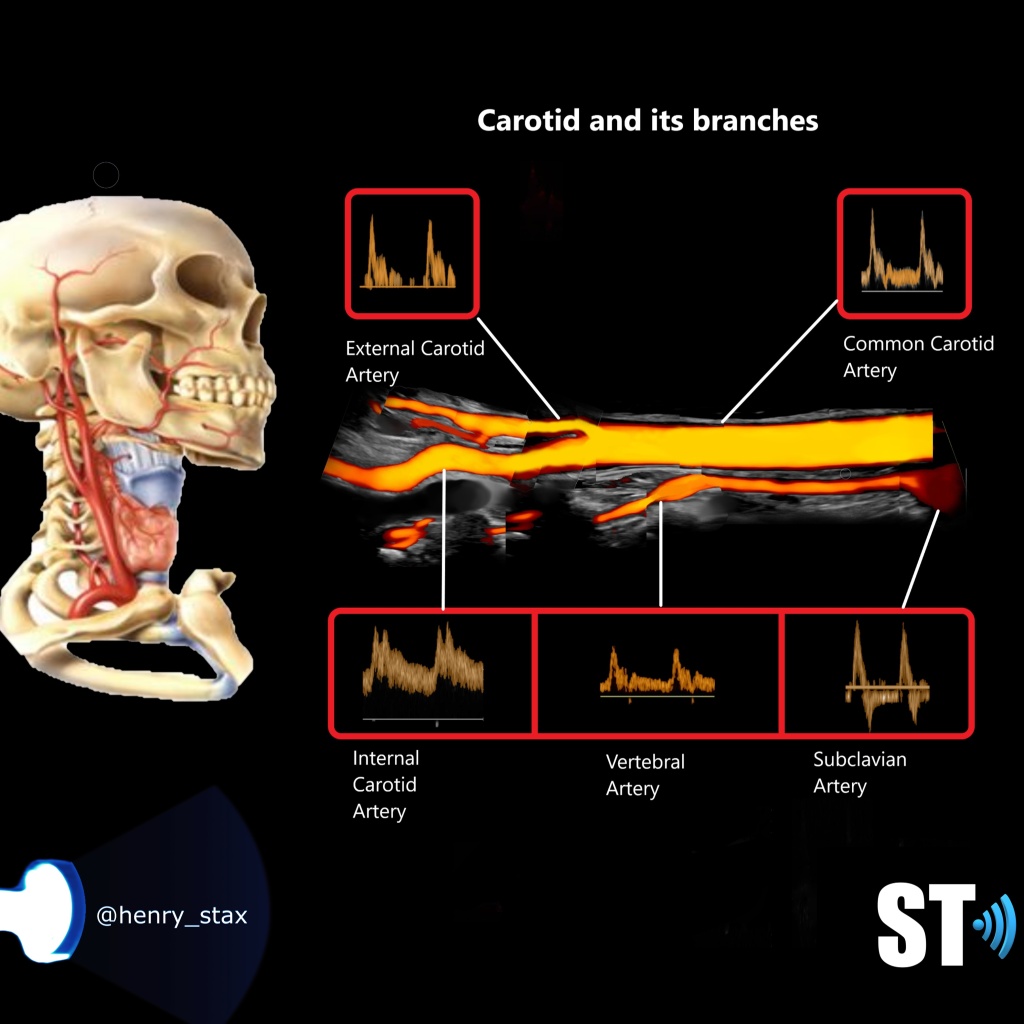
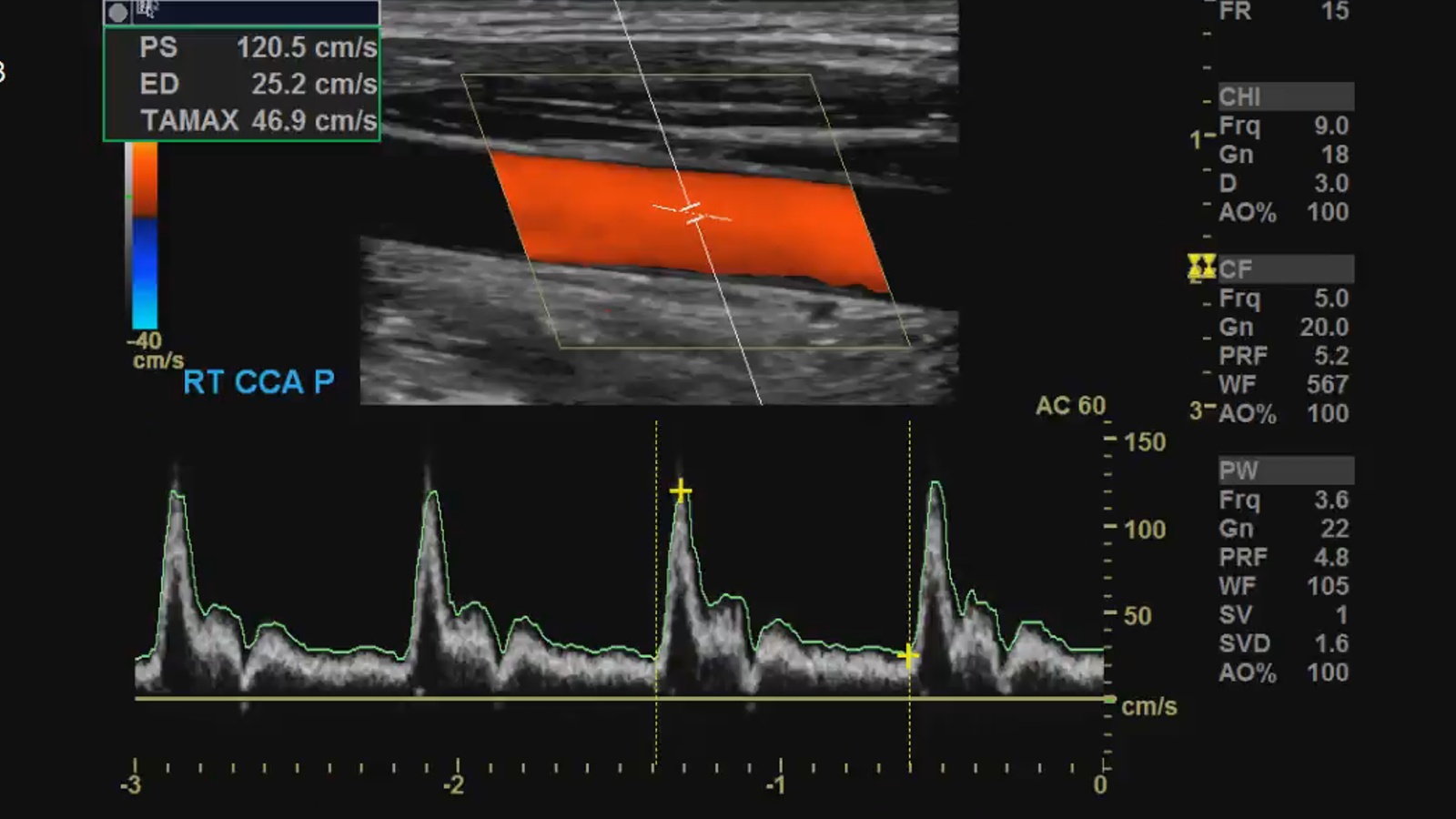
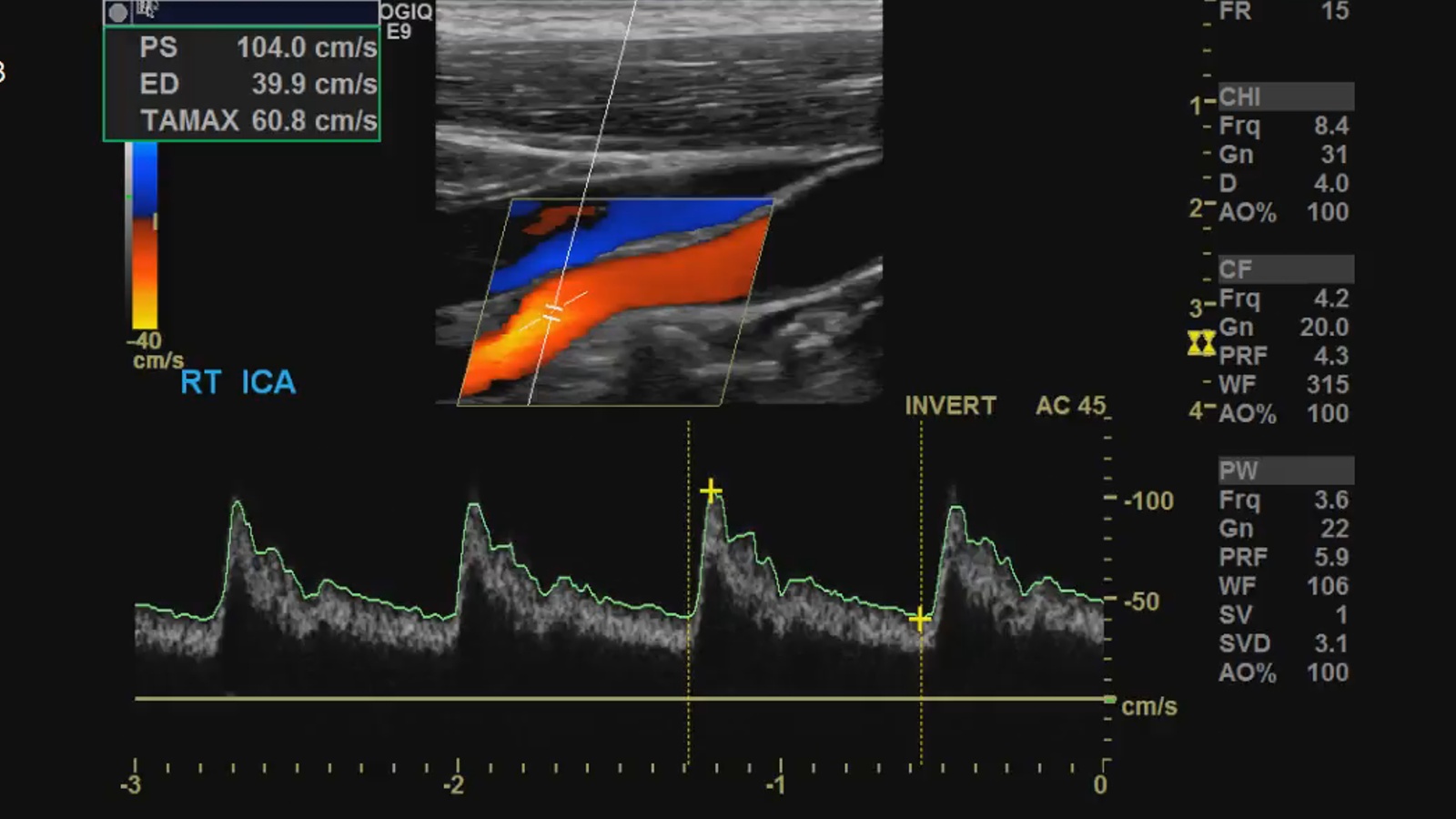
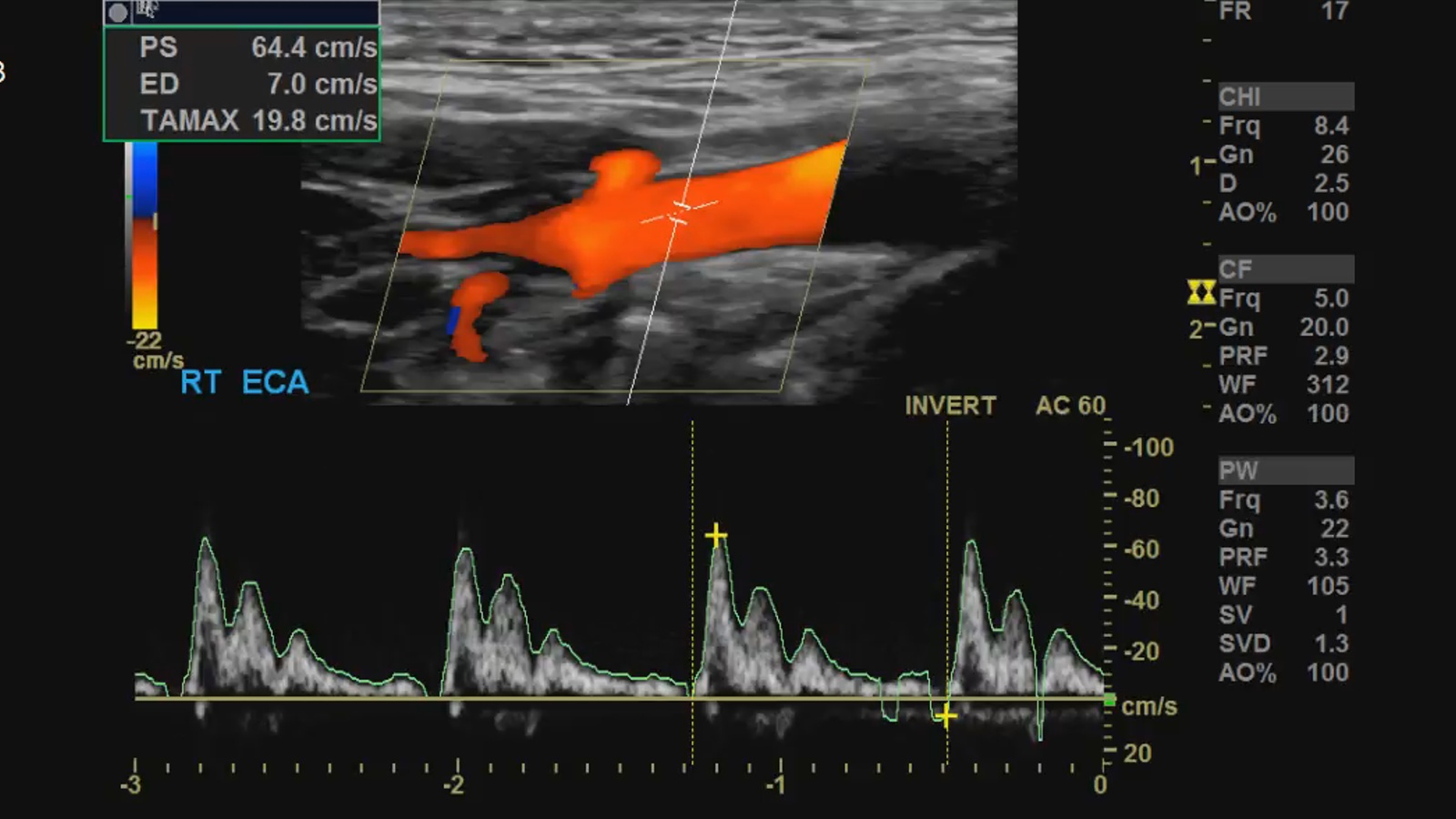
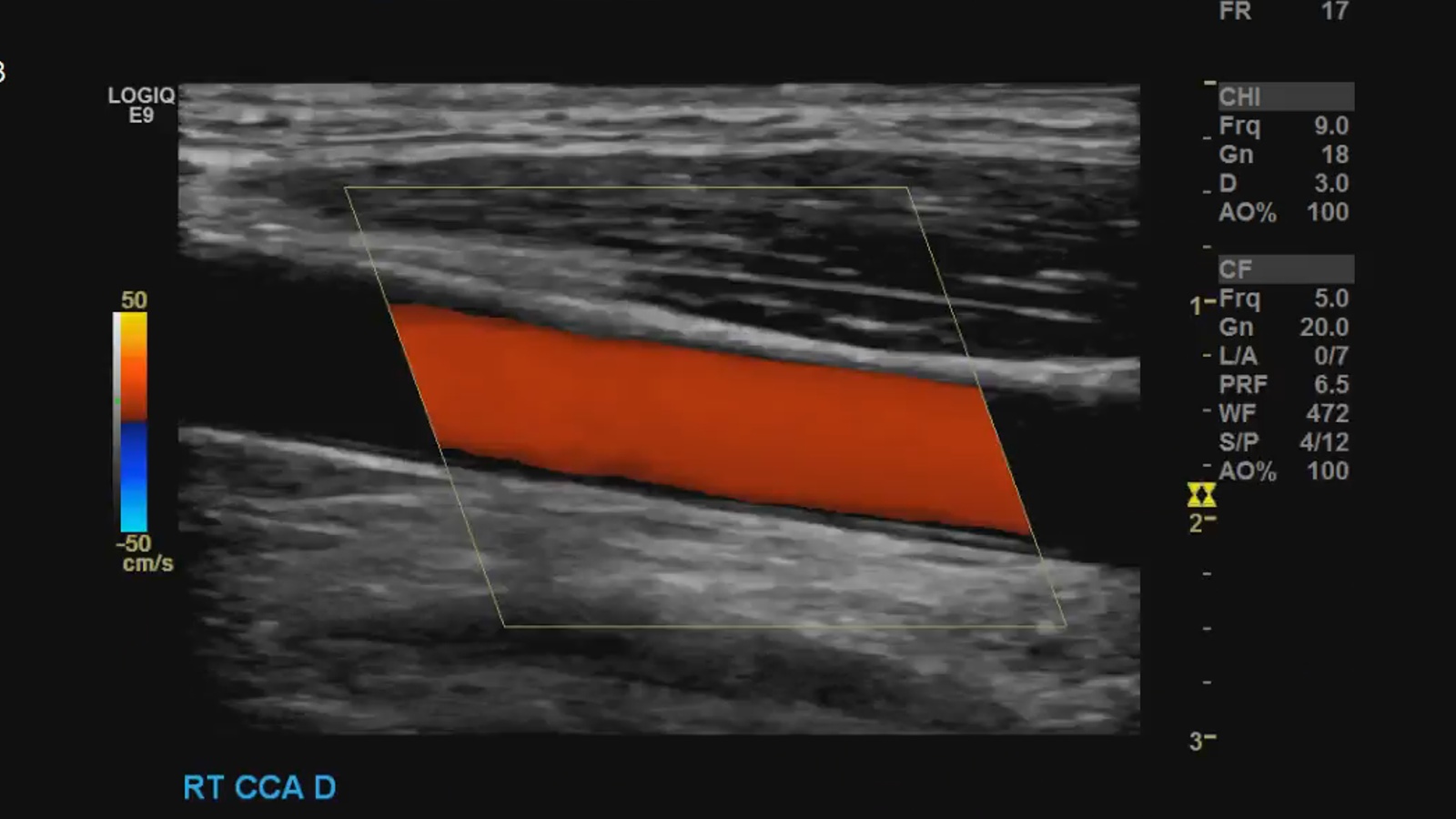
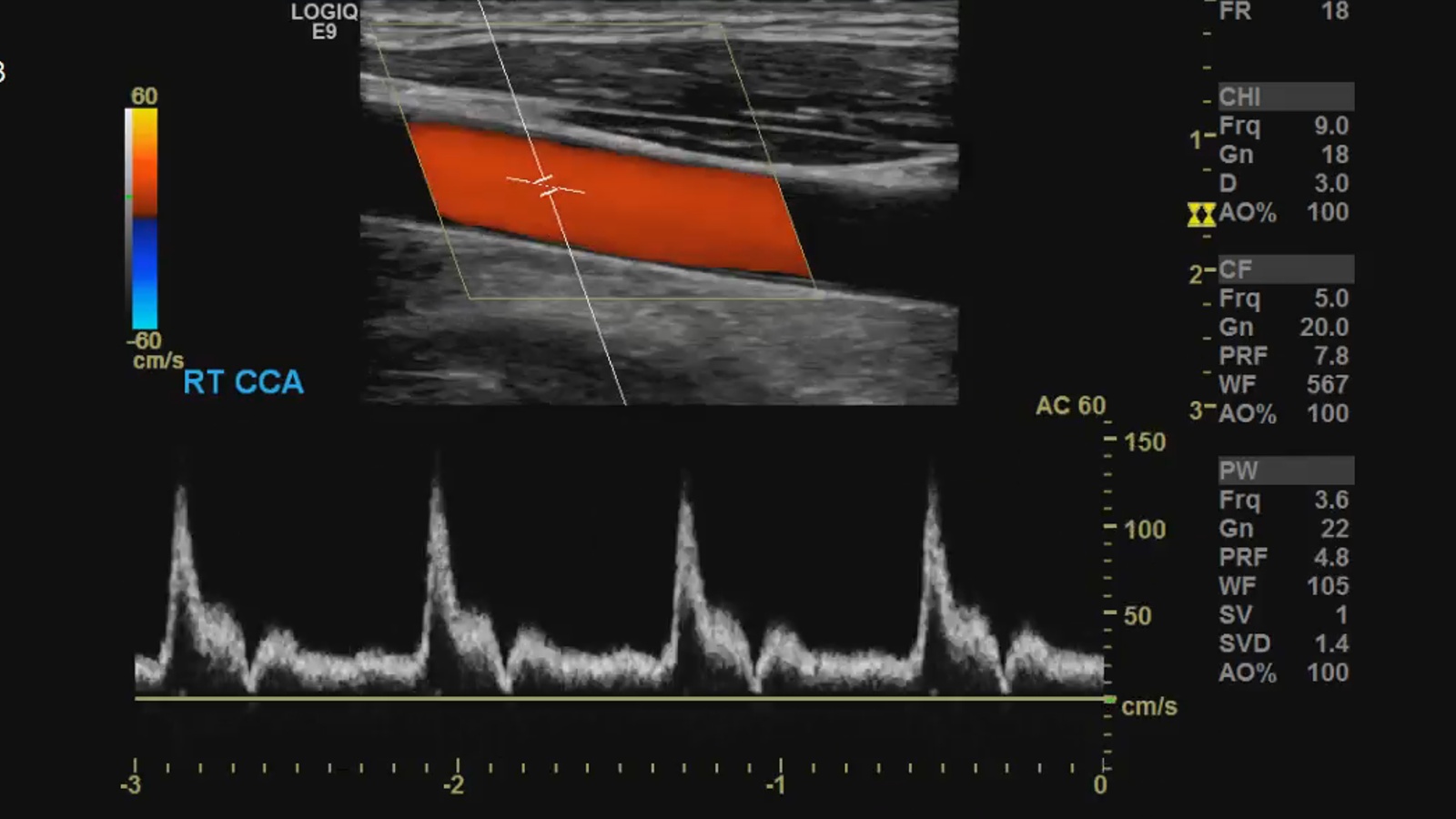
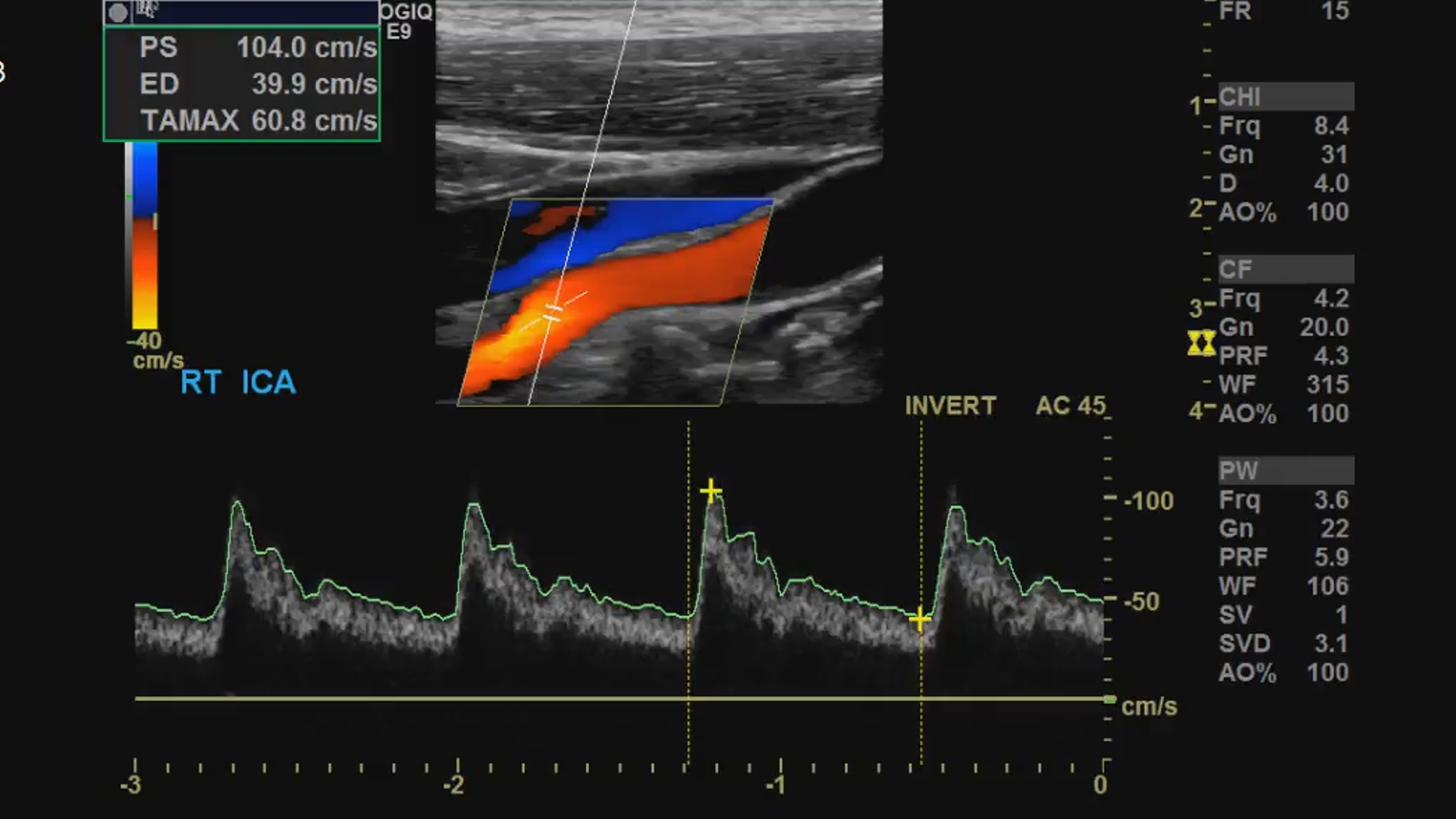
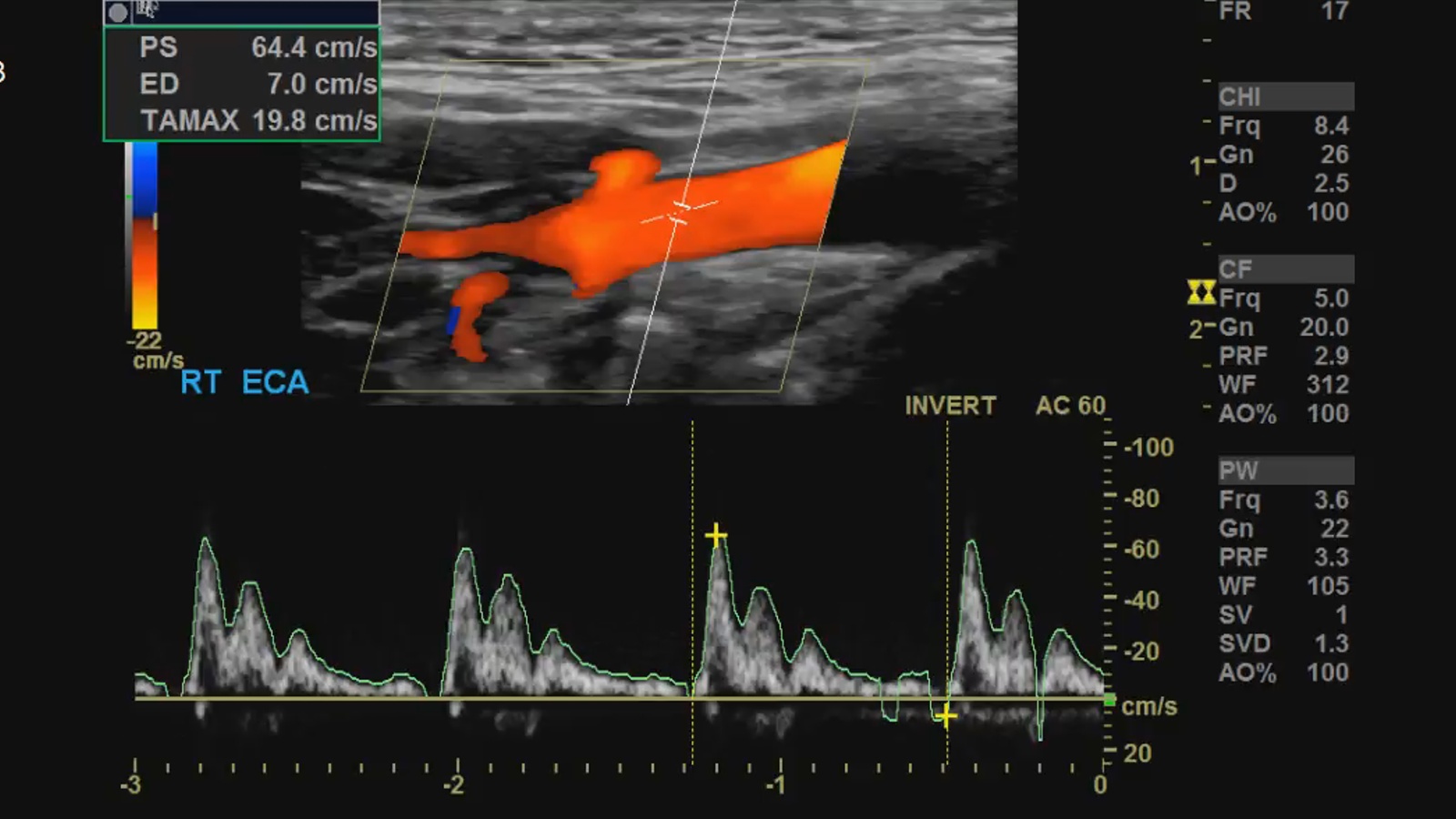
In normal arteries flow is described as laminar, which means the blood cells move parallel to the vessel walls, which is faster in the center than at near the wall which is attributed to friction. AKA parabolic flow. Though flow in the CCA is usually laminar this is not true of the Bulb and tortuous vessels. As far as spectral Doppler is concerned, there is a difference of pulsatility depending on what vessel is being interrogated, CCA having a sharp upstroke and decent amount of diastolic flow, ICA has a broad upstroke and considerable diastolic flow, and ECA having A very sharp upstroke and little to no diastolic flow with reversal of flow in some patients.
Techniques
- Beam steering needs to be done in a direction that allows the smallest angles of incidence to blood flow.
- Scale/Pulse Repetition Frequency PRF
- Higher velocities – increase PRF to avoid aliasing
- Lower velocities – decrease PRF to optimize color filling
3.Gain needs to be setup in order to achieve good color filling without inducing speckle artifacts, but not to low that the vessels underfill.
4. Color box and spectral gate size should be big enough for the area of interest
5. Spectral Doppler angle should be from 45 – 60 degrees to avoid overestimation of velocities
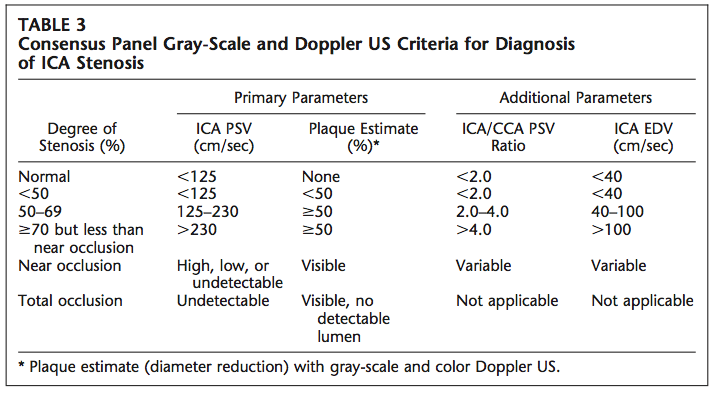
6. ICA/CCA ratio is the Peak systolic velocity (PSV) of the CCA divided by the PSV of the ICA a ICA/CCA PSV ratio < 2.0 is indicative of a <50% stenosis i.e. Unremarkable exam with no “hemodynamically significant stenosis”.
Protocol
According to the AIUM, a minimum of CCA, Bulb and BIF, ICA, ECA and VA should be scanned with grayscale, color Doppler and spectral Doppler. [4]
Now protocols vary from institution to institution, however, most places follow these guidelines. I will show you my protocol.
Begin with the
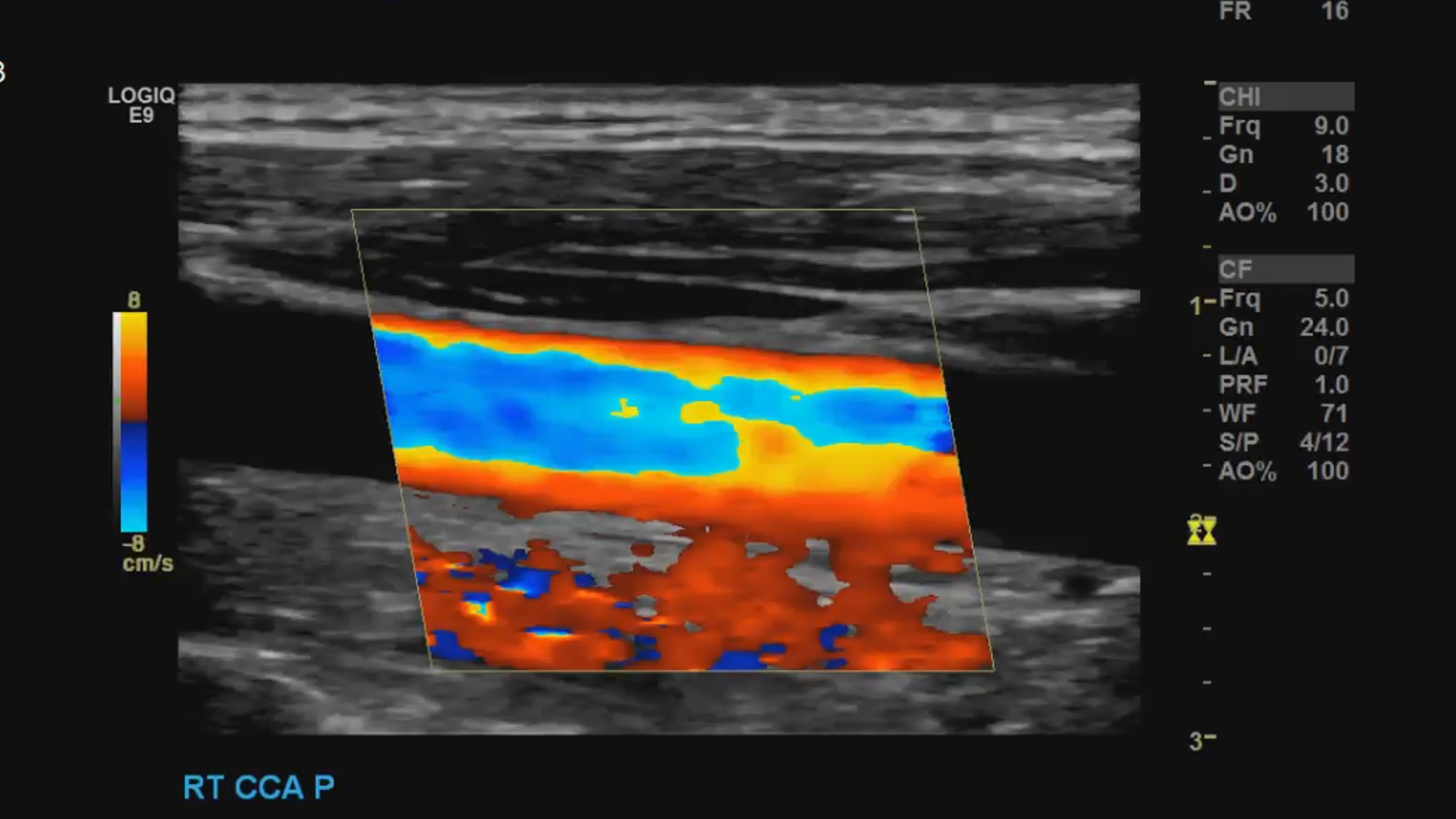
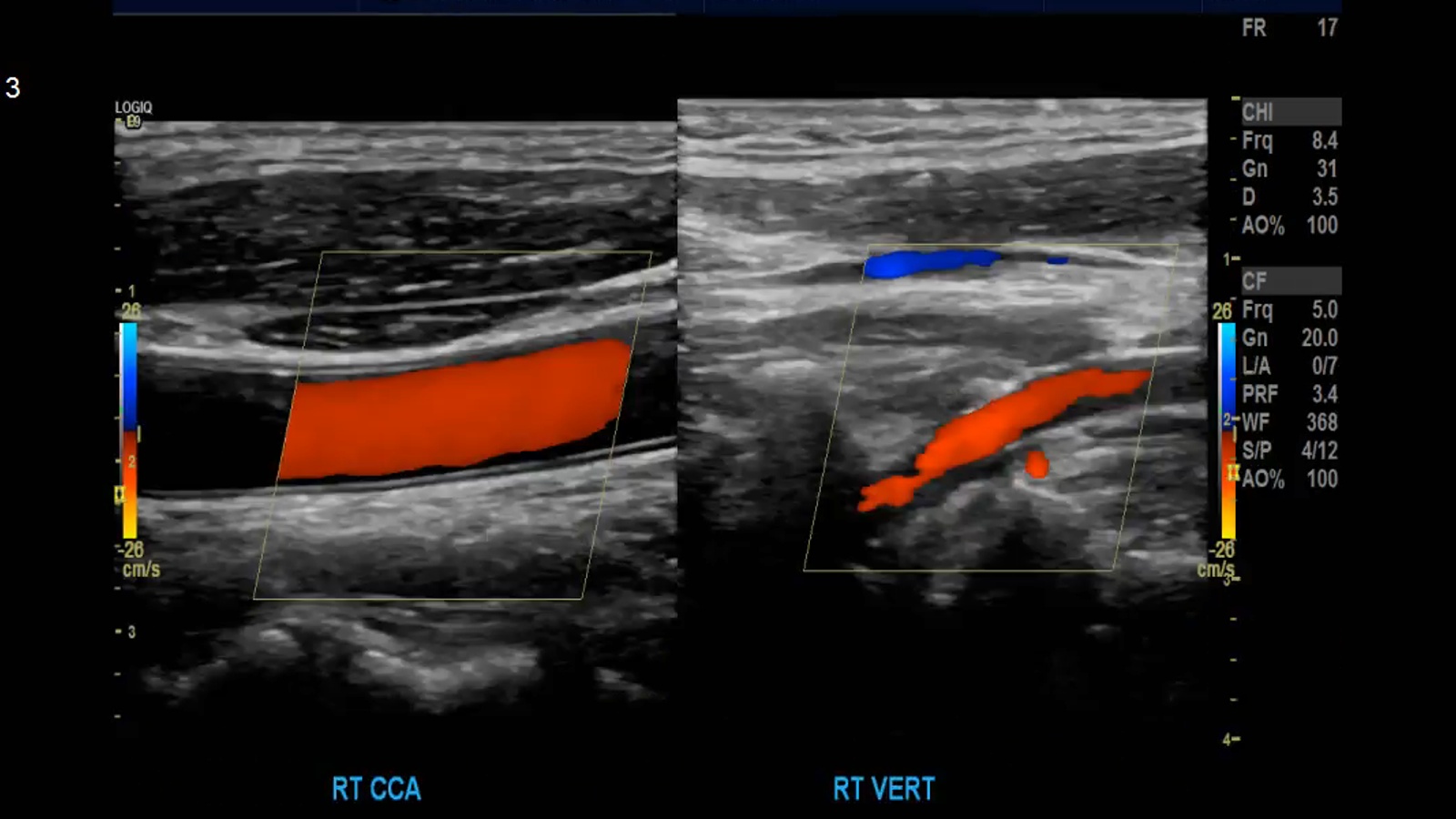
CCA proximal in transverse; greyscale and color Doppler
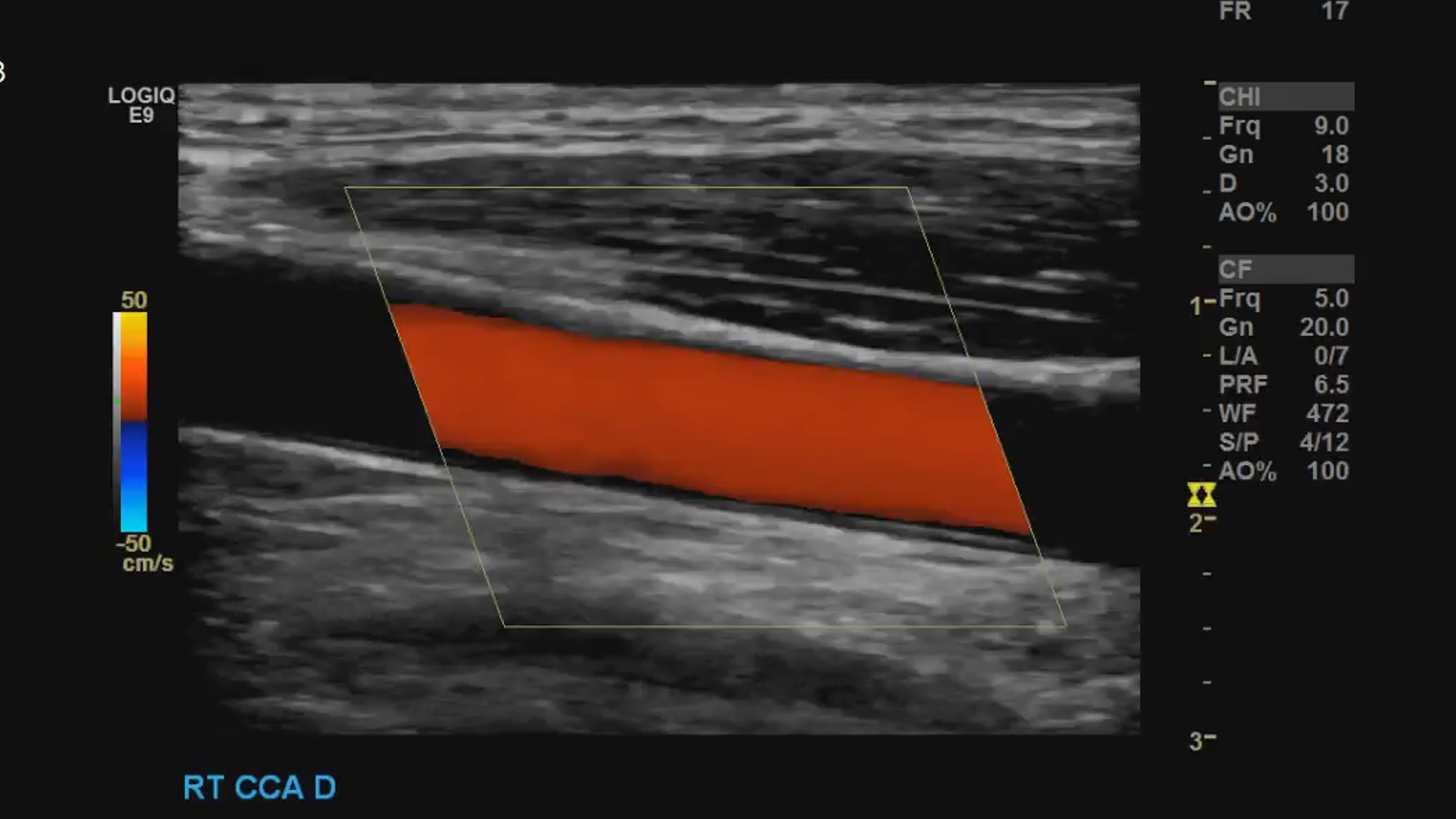
Sagittal grayscale, color and spectral Doppler with measurements PSV and EDV.
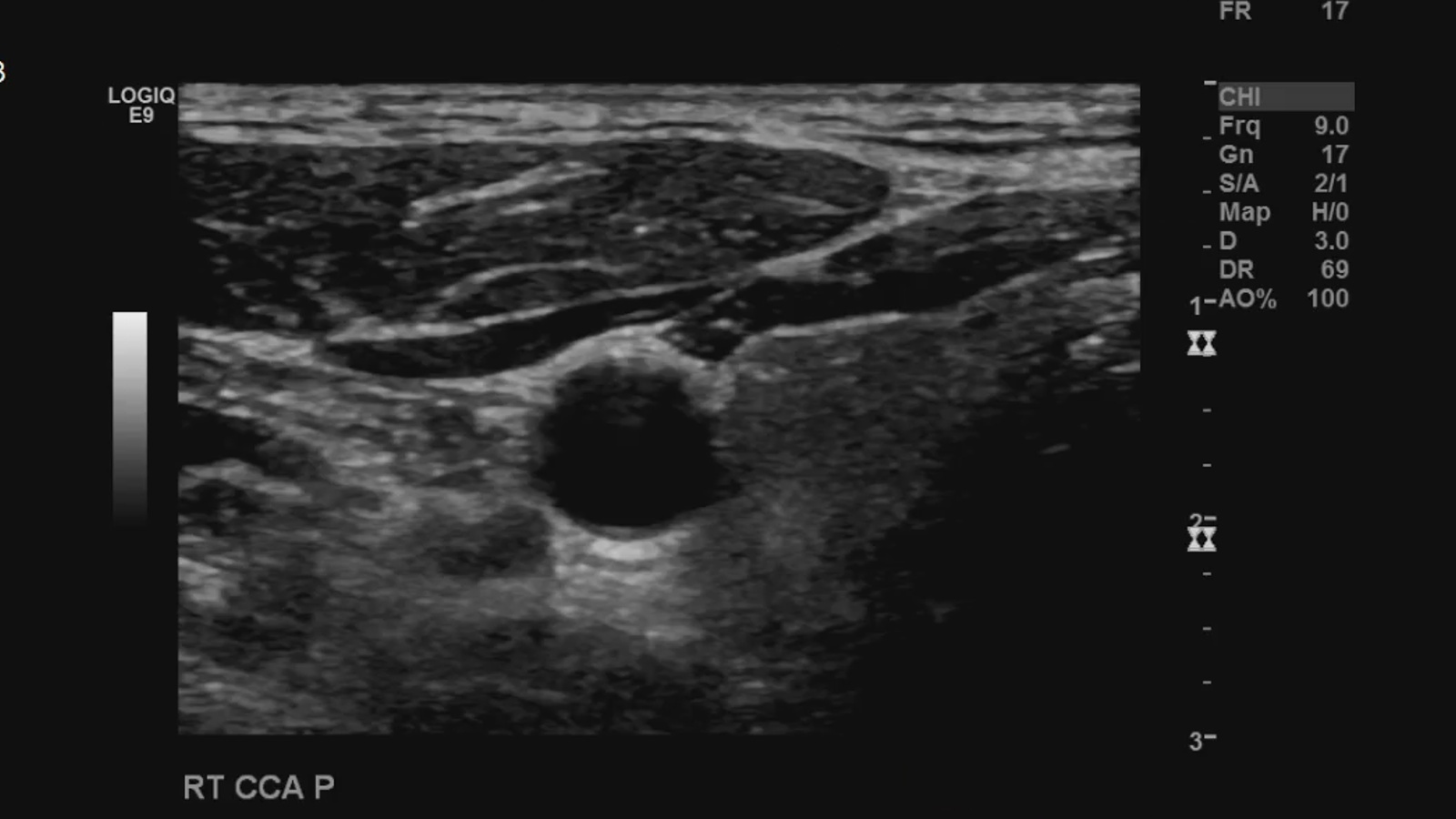
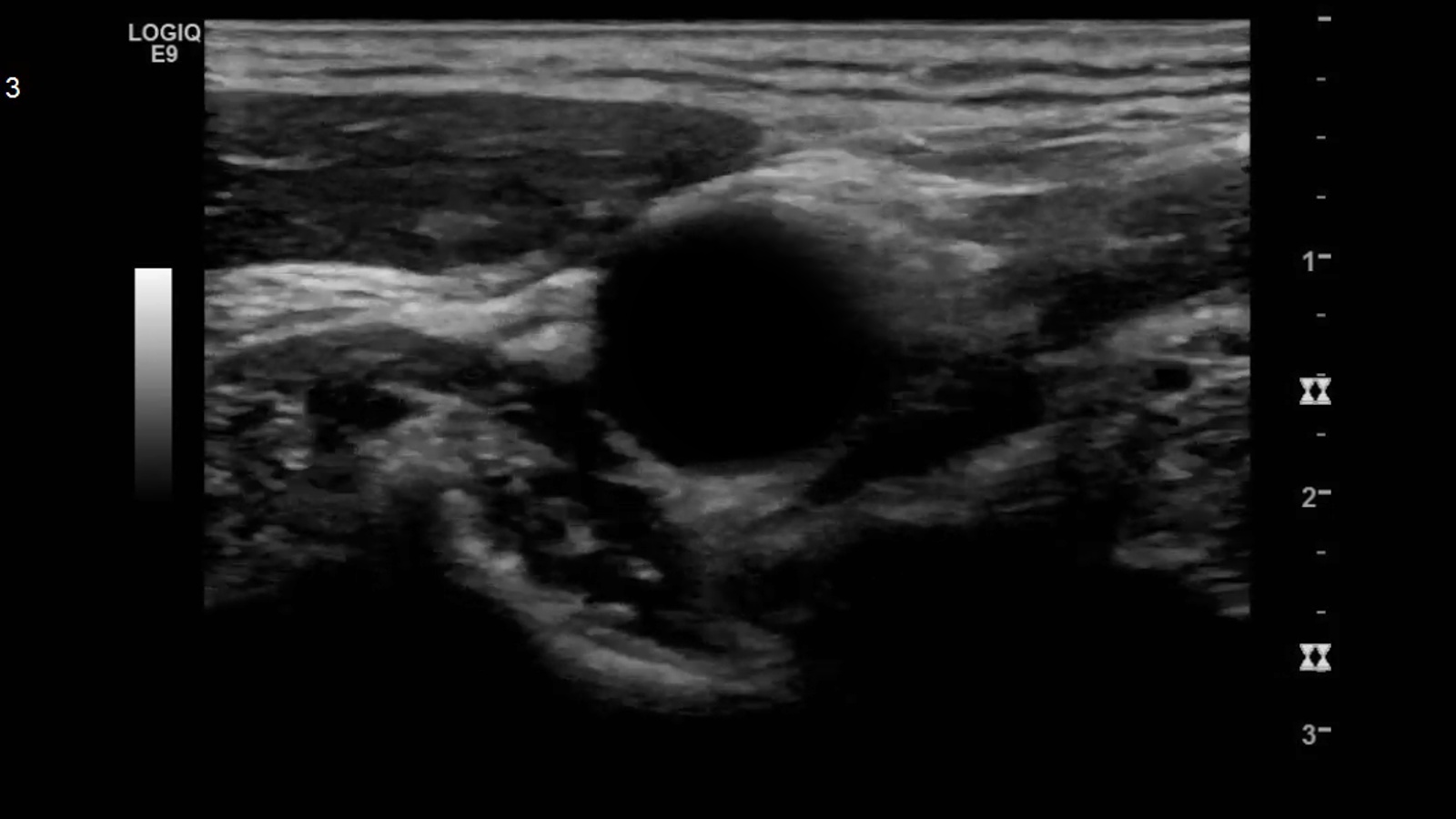
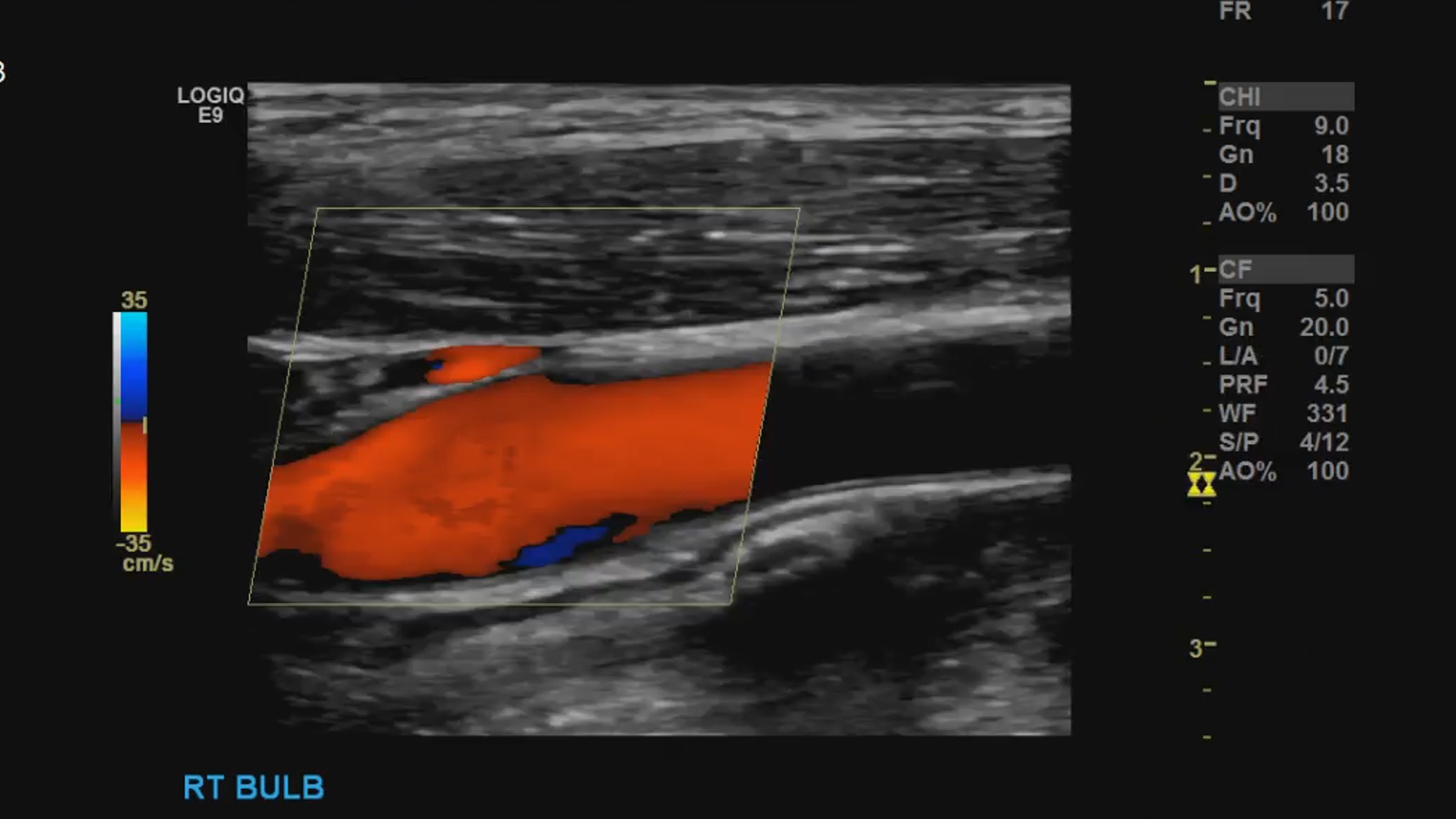
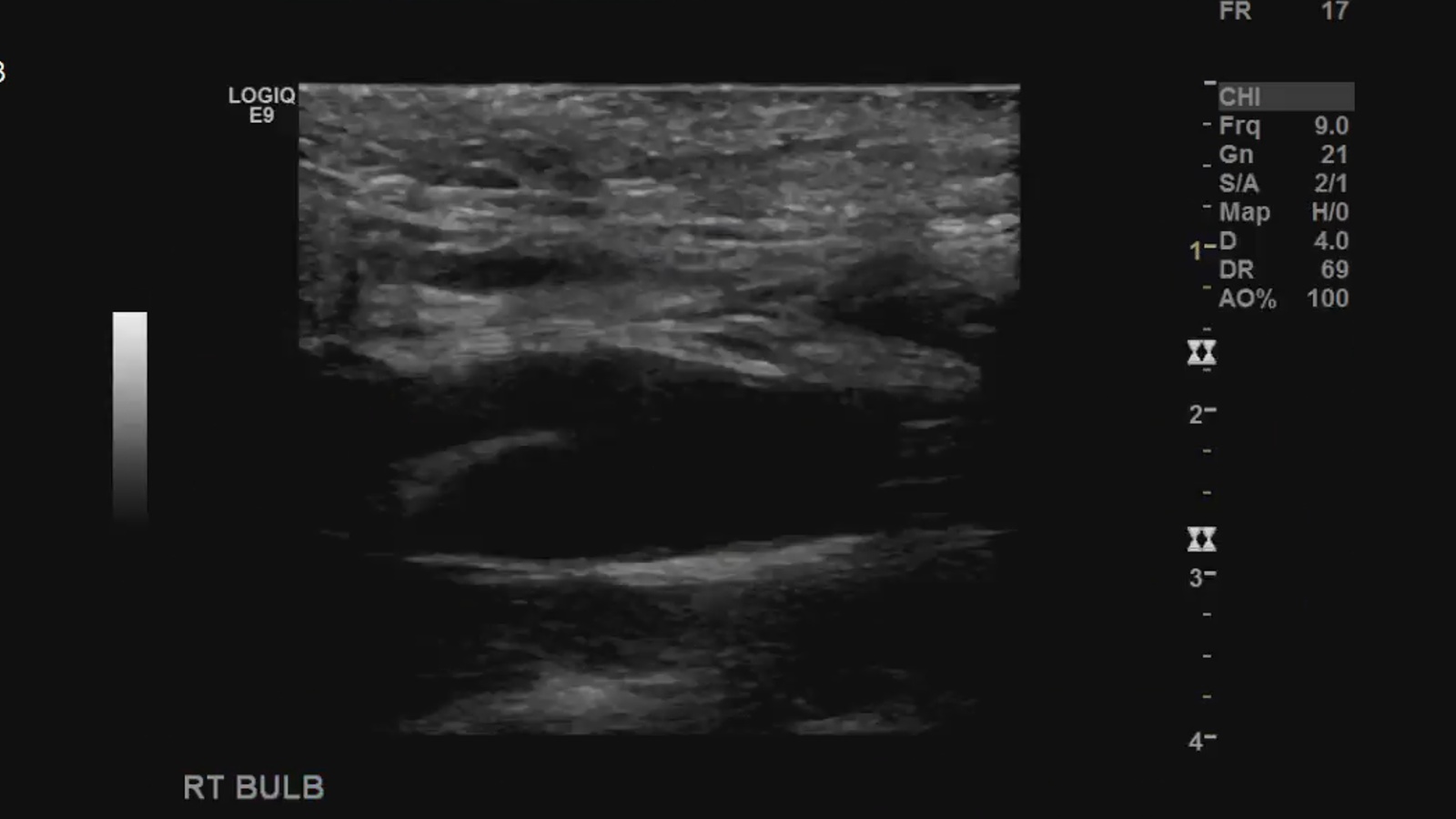
CCA bulb in transverse; greyscale and color Doppler
Sagittal grayscale, color and spectral Doppler.

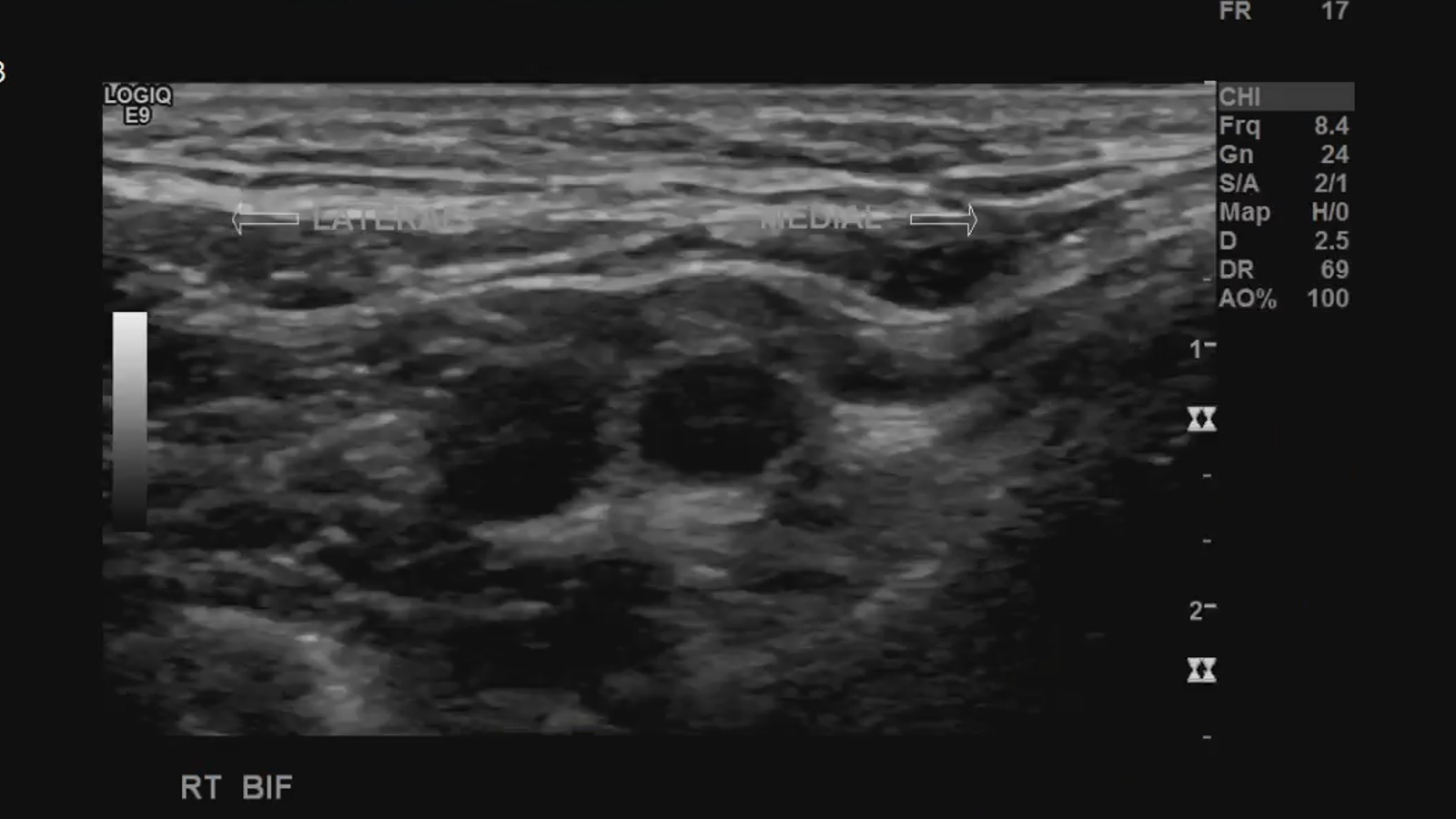
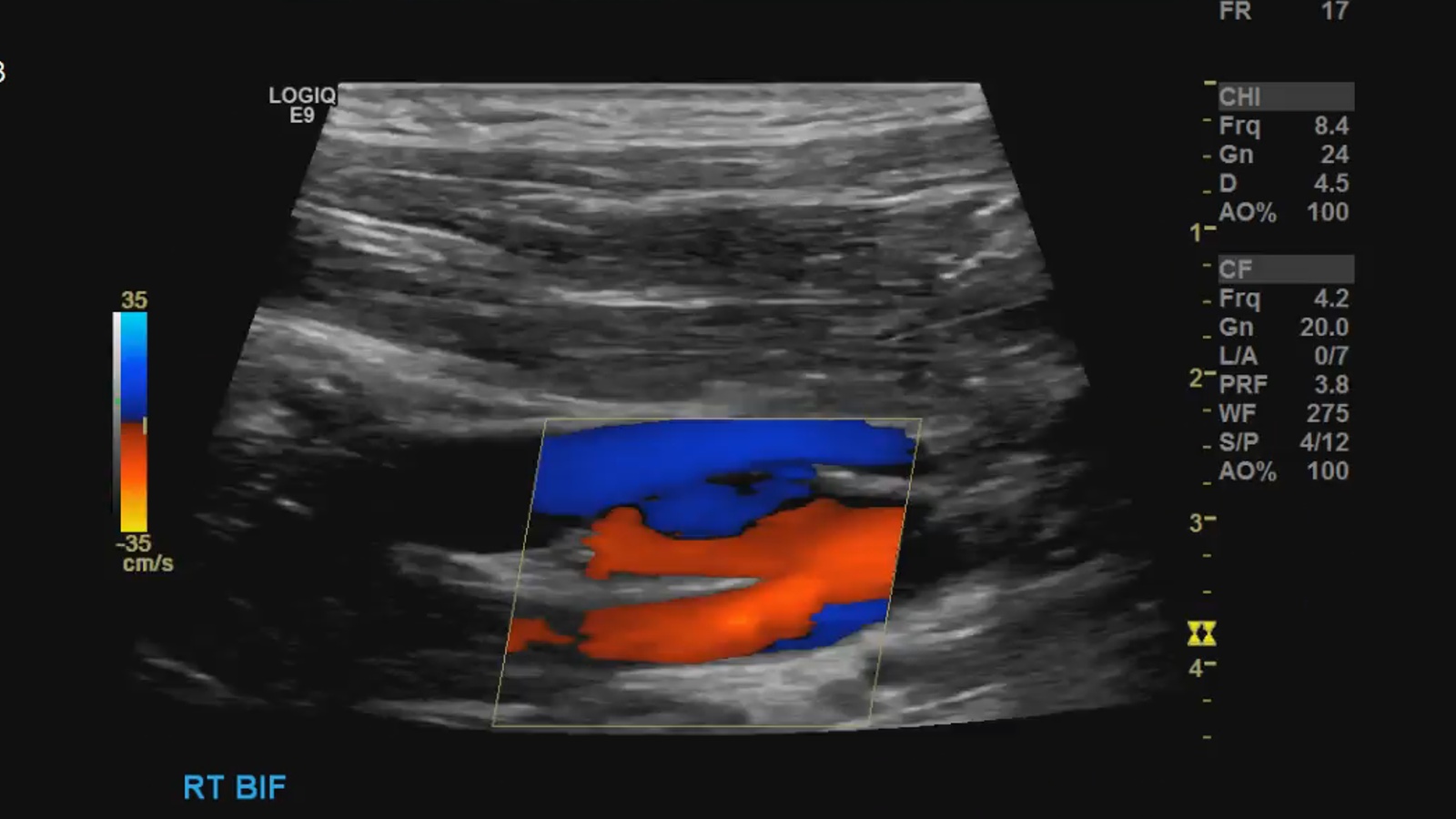
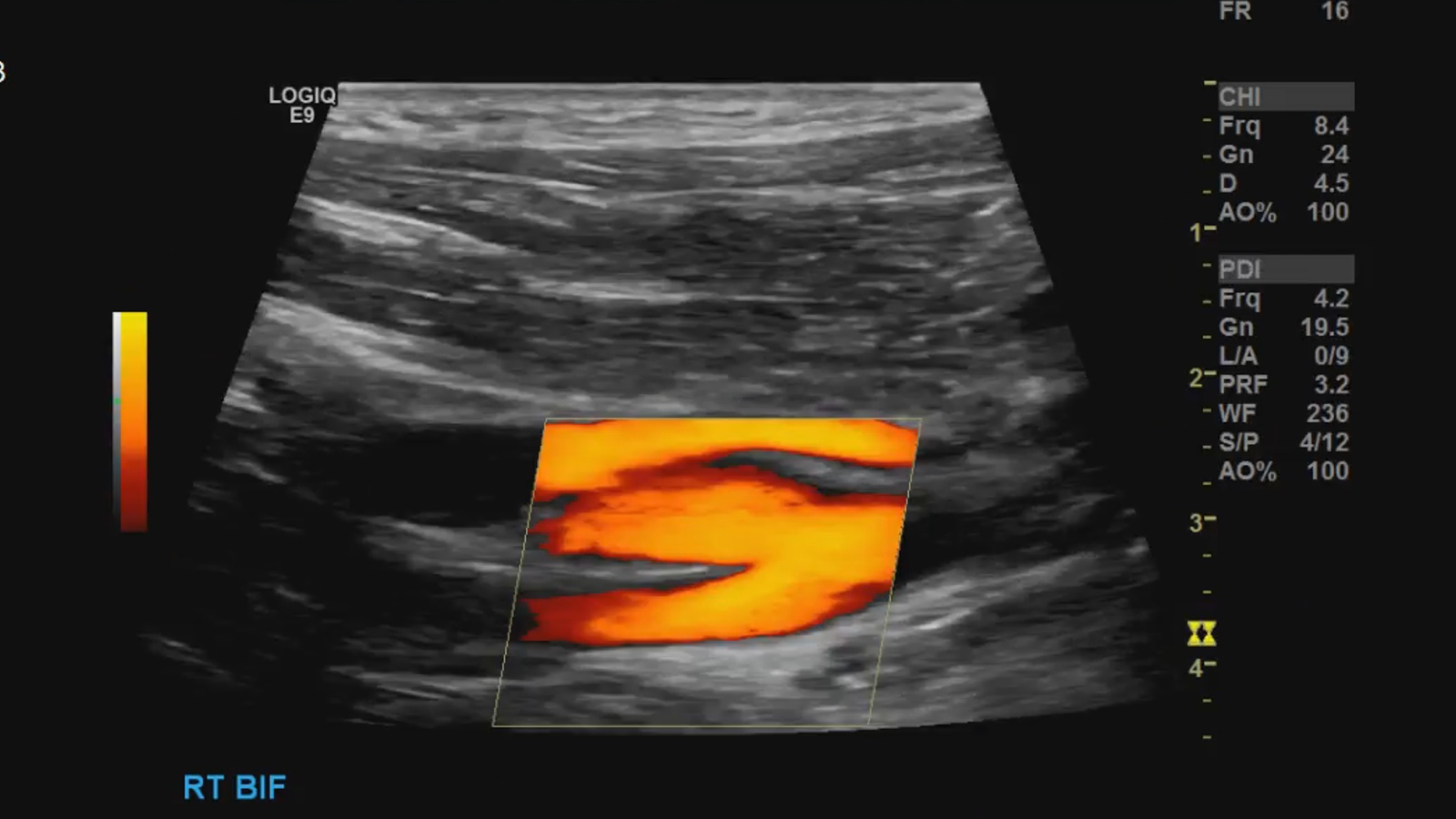
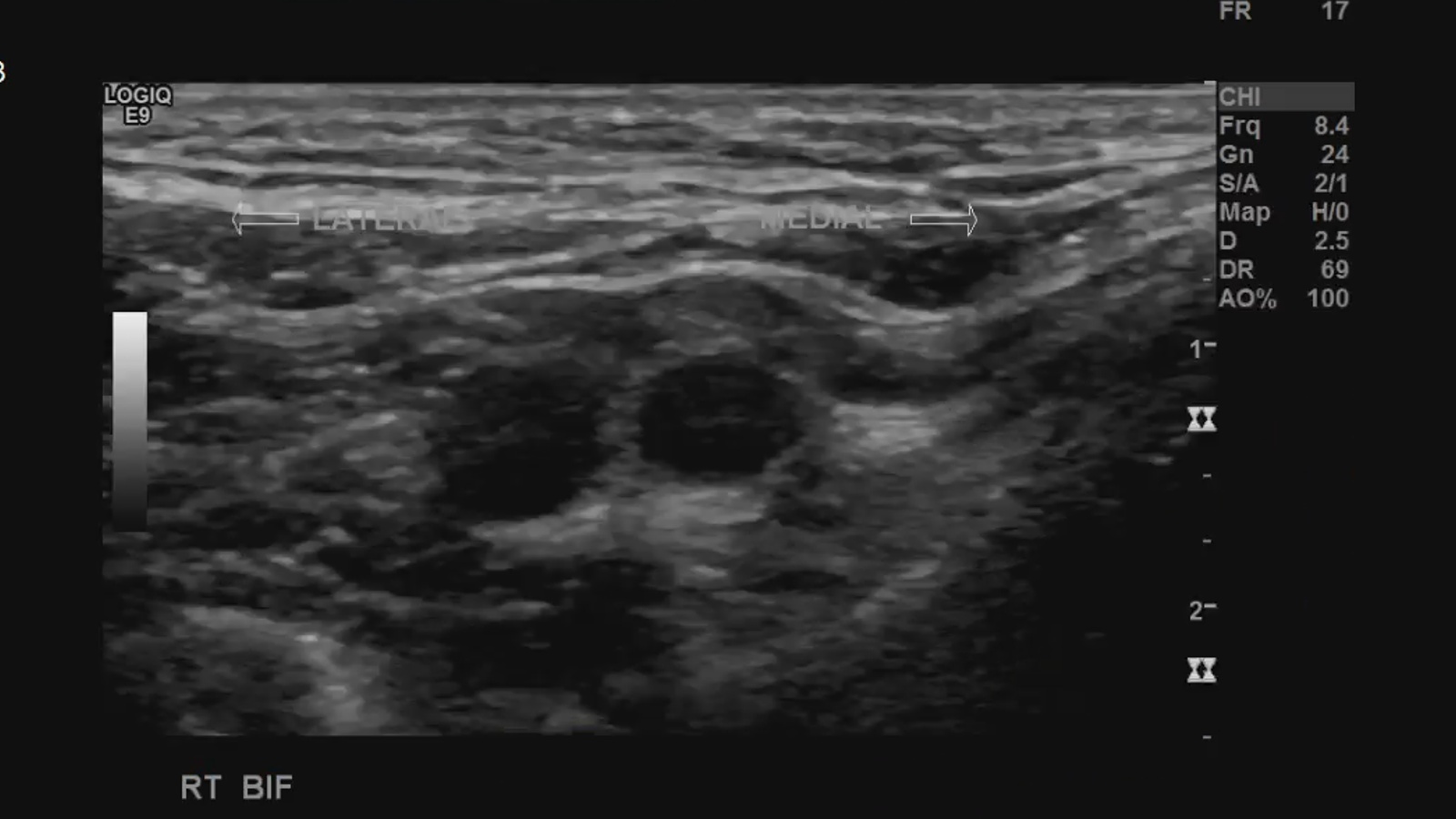
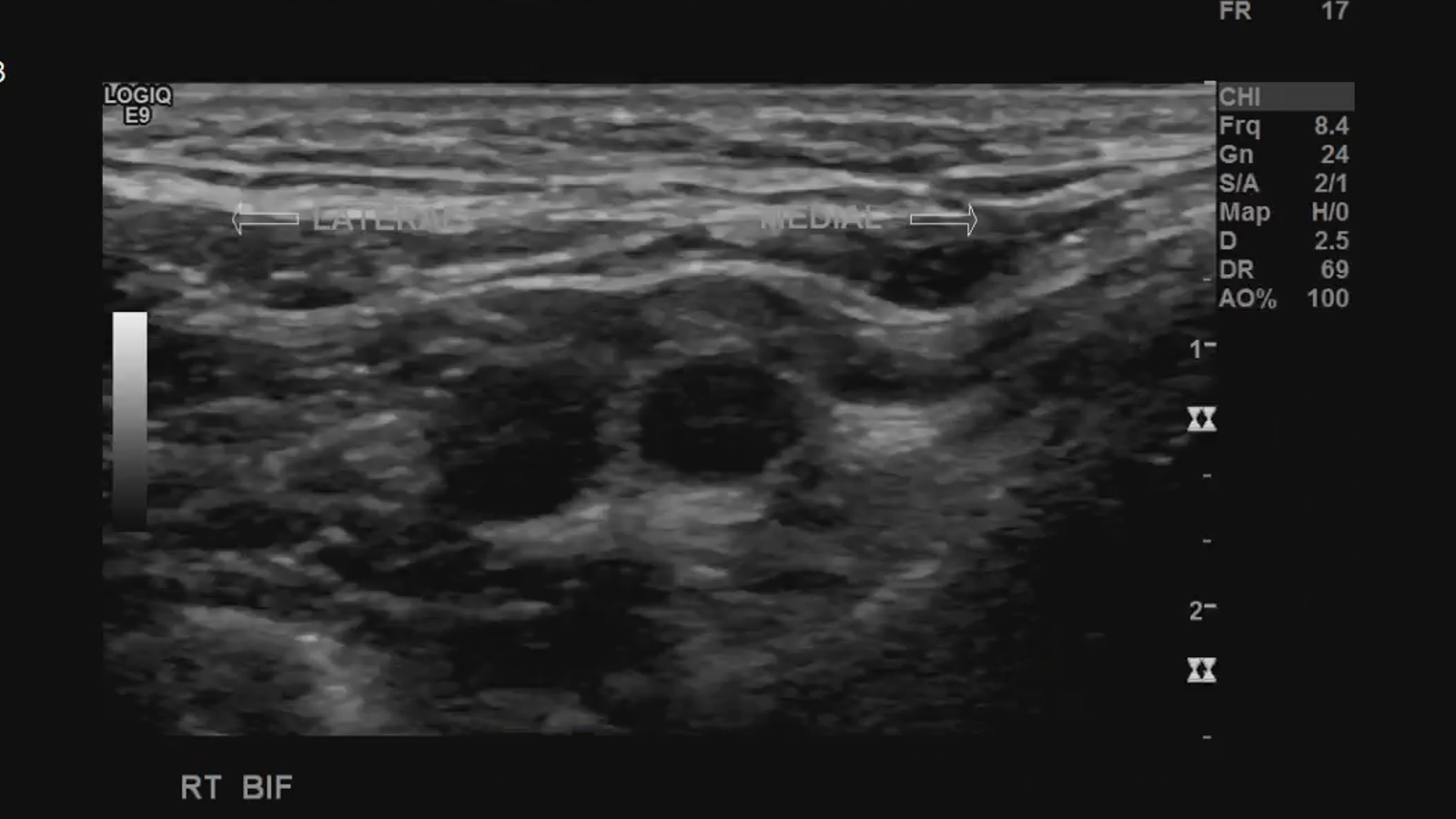
Bifurcation in transverse; greyscale and color Doppler
Sagittal grayscale, color and spectral Doppler.
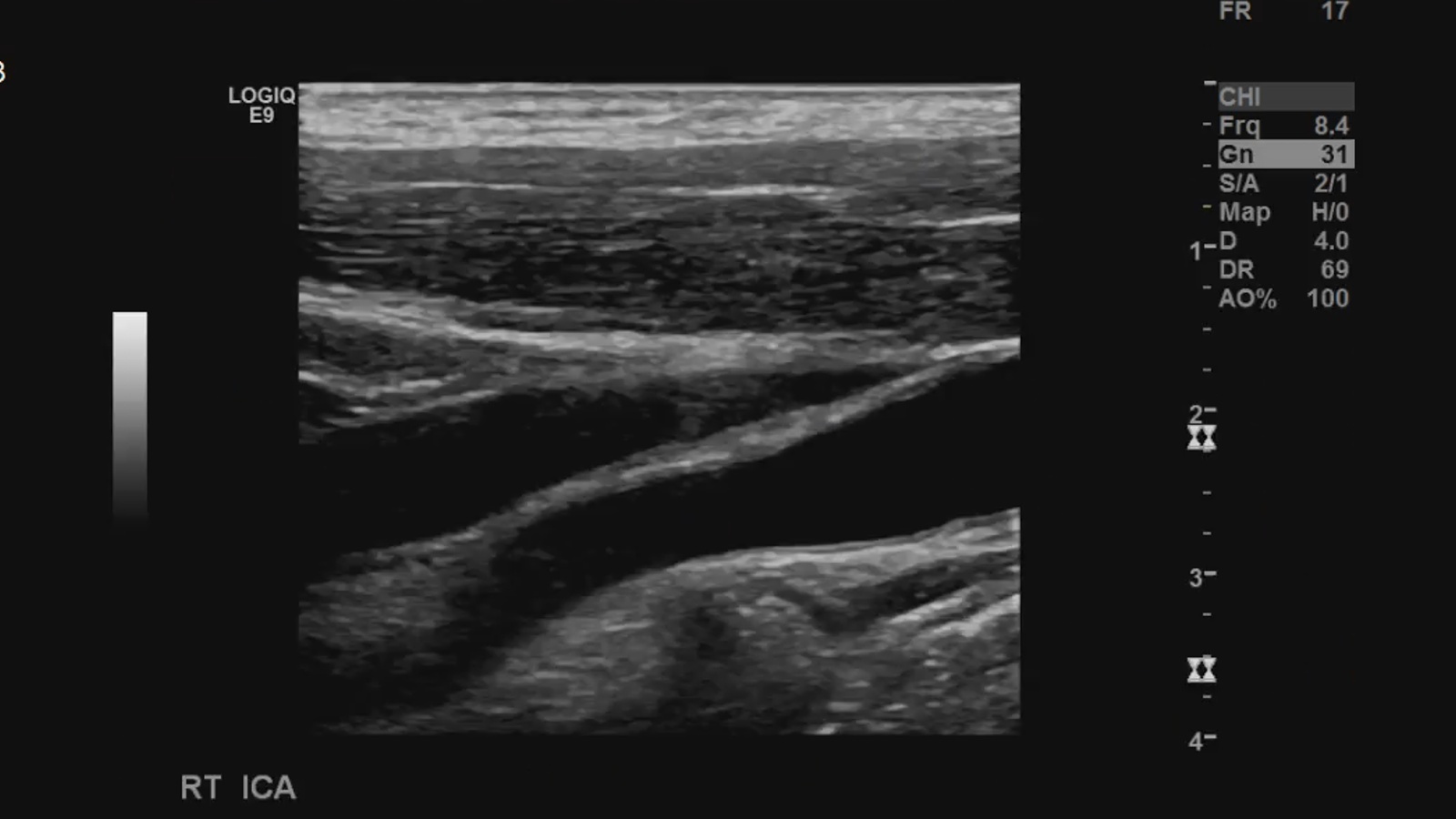
ICA in transverse; greyscale and color Doppler
Proximal Sagittal grayscale, color and spectral Doppler.
Mid sagittal grayscale, color and spectral Doppler.
Distal sagittal grayscale, color and spectral Doppler.
with measurements PSV and EDV on all 3
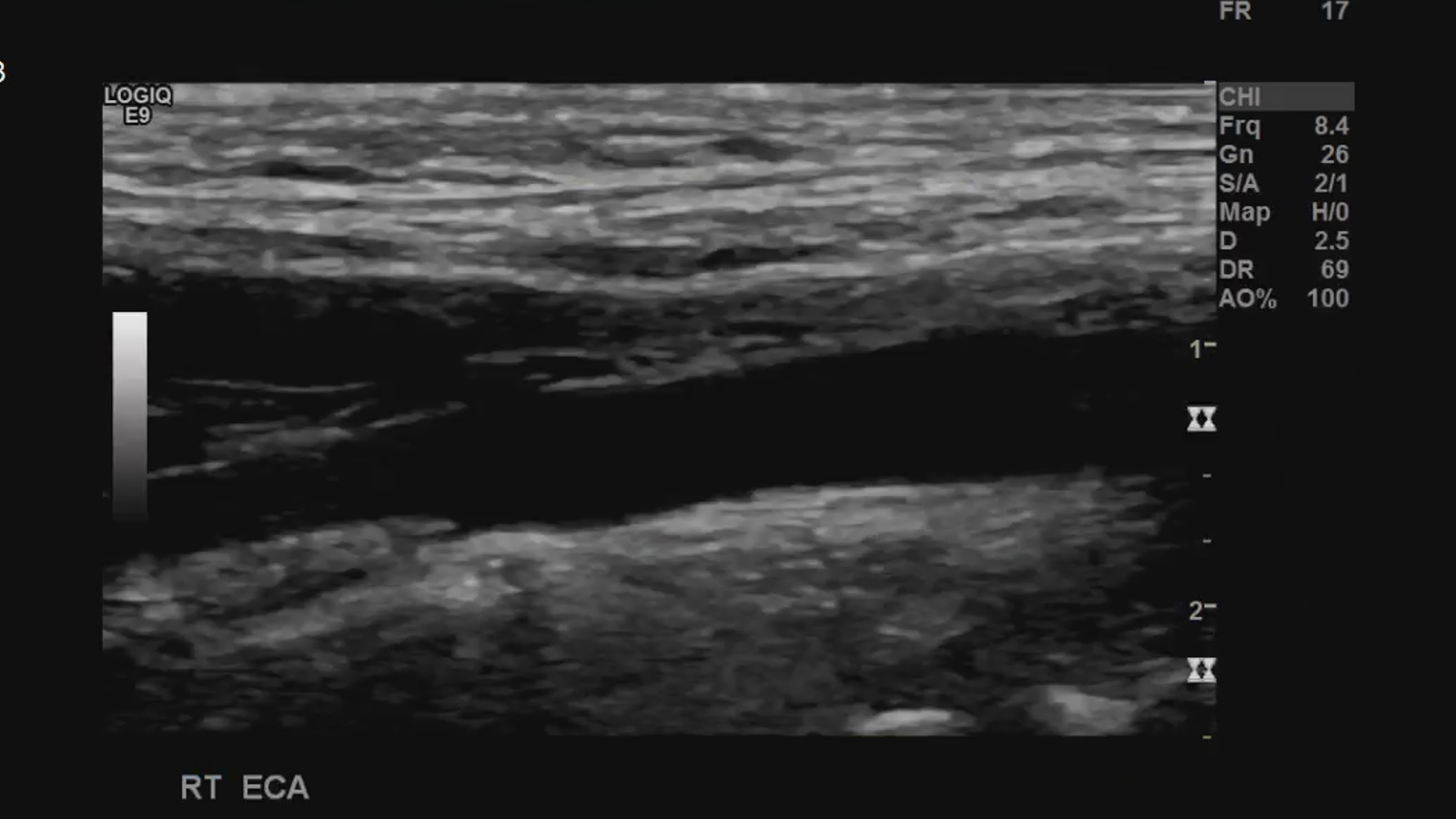
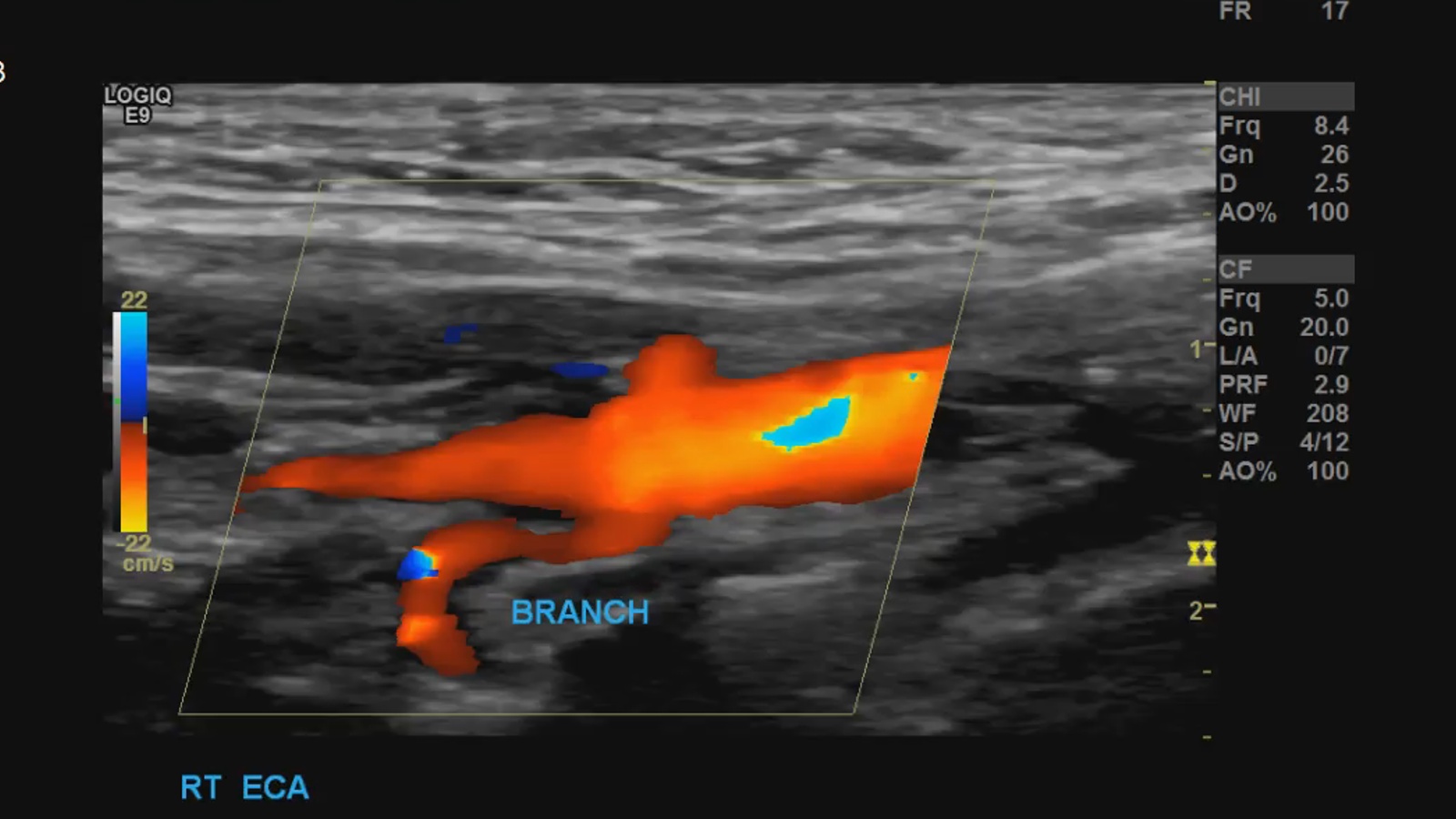
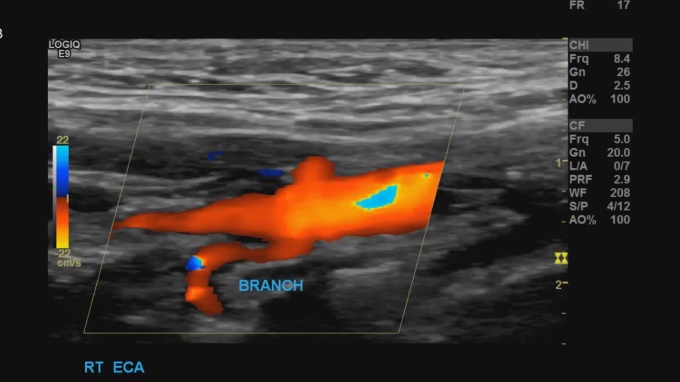
ECA in transverse; greyscale and color Doppler
Proximal Sagittal show branches
grayscale, color and spectral Doppler with measurements PSV.
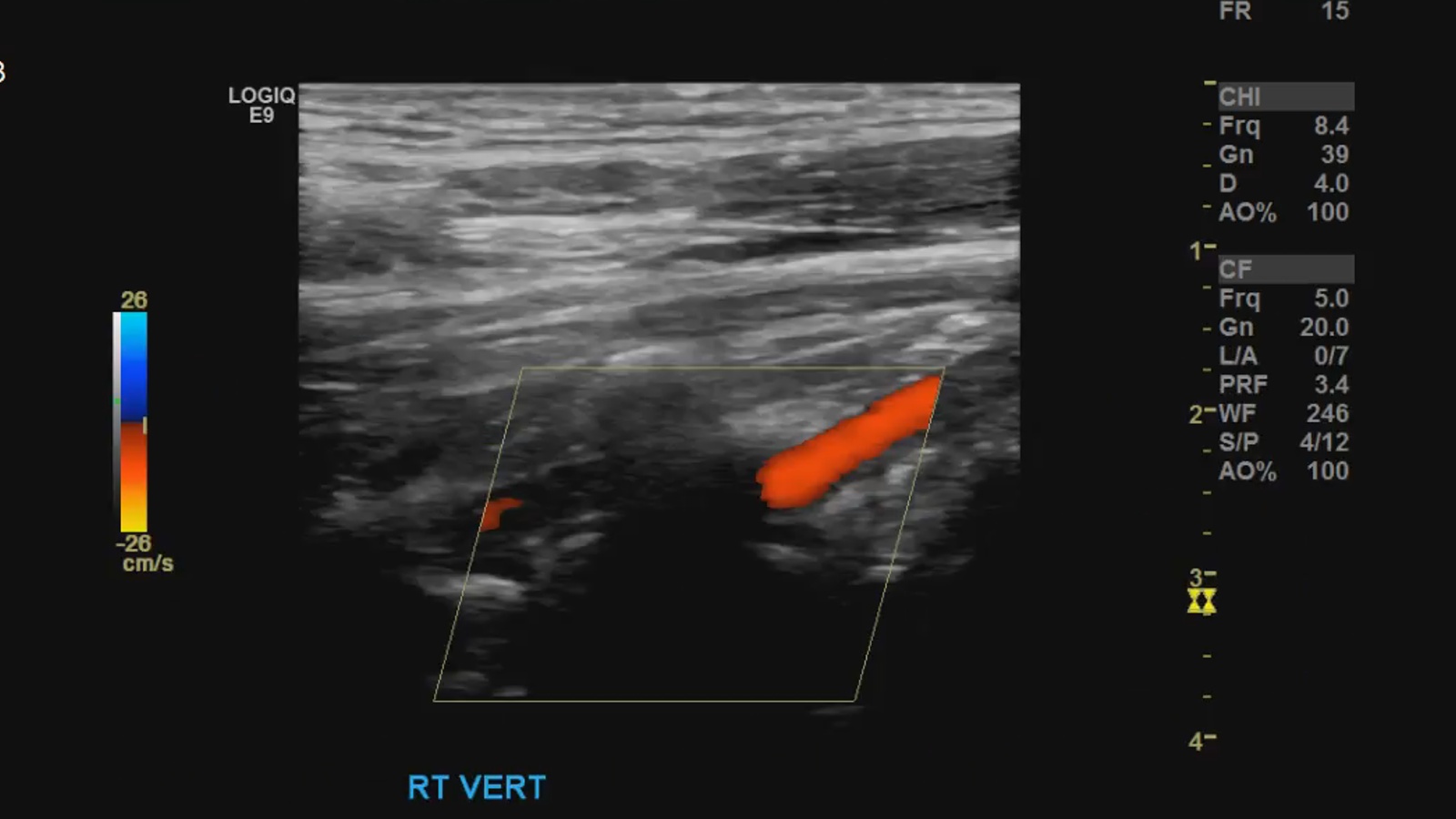
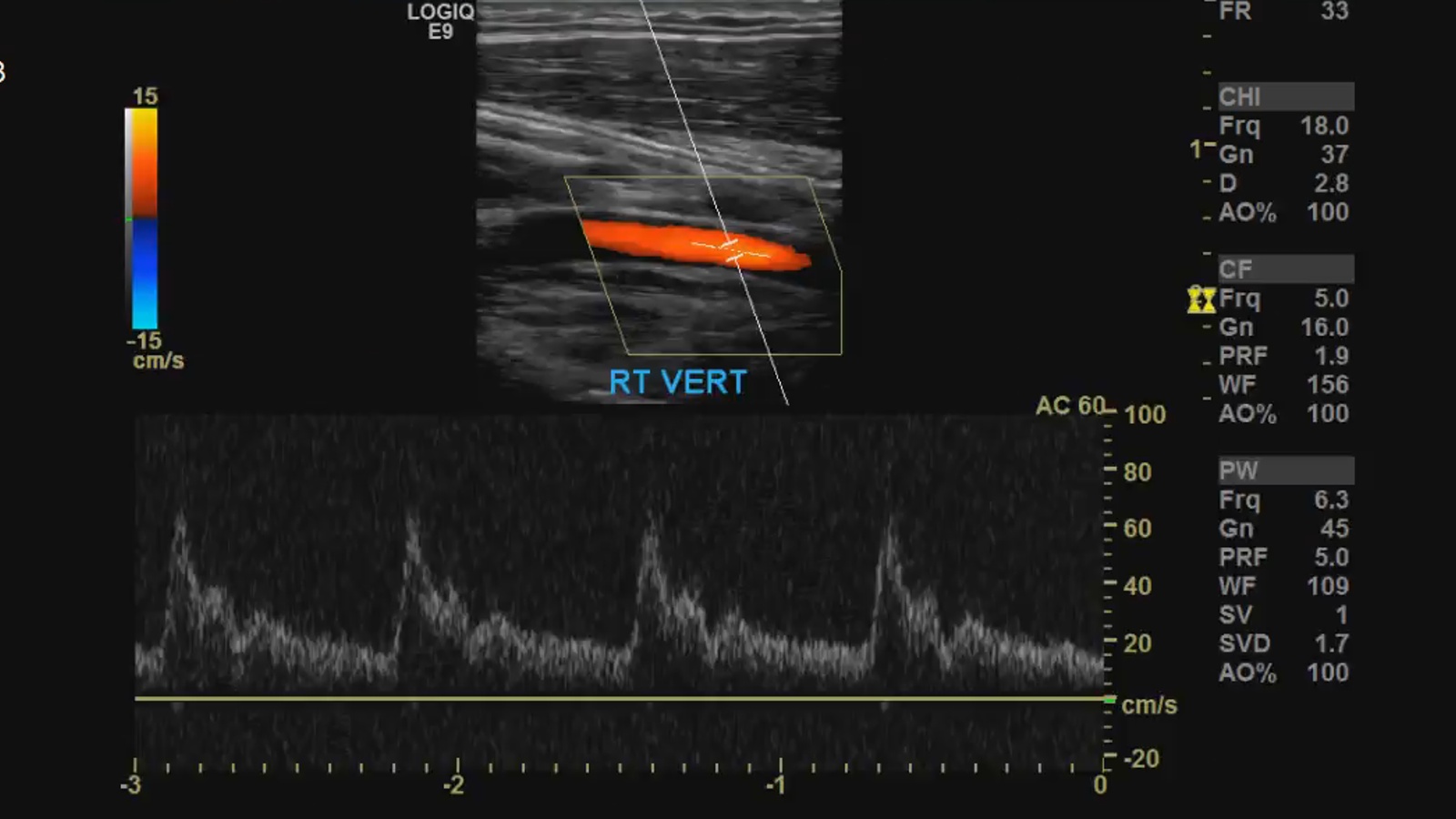
VA Sagittal grayscale, color and spectral Doppler with measurements PSV and EDV.
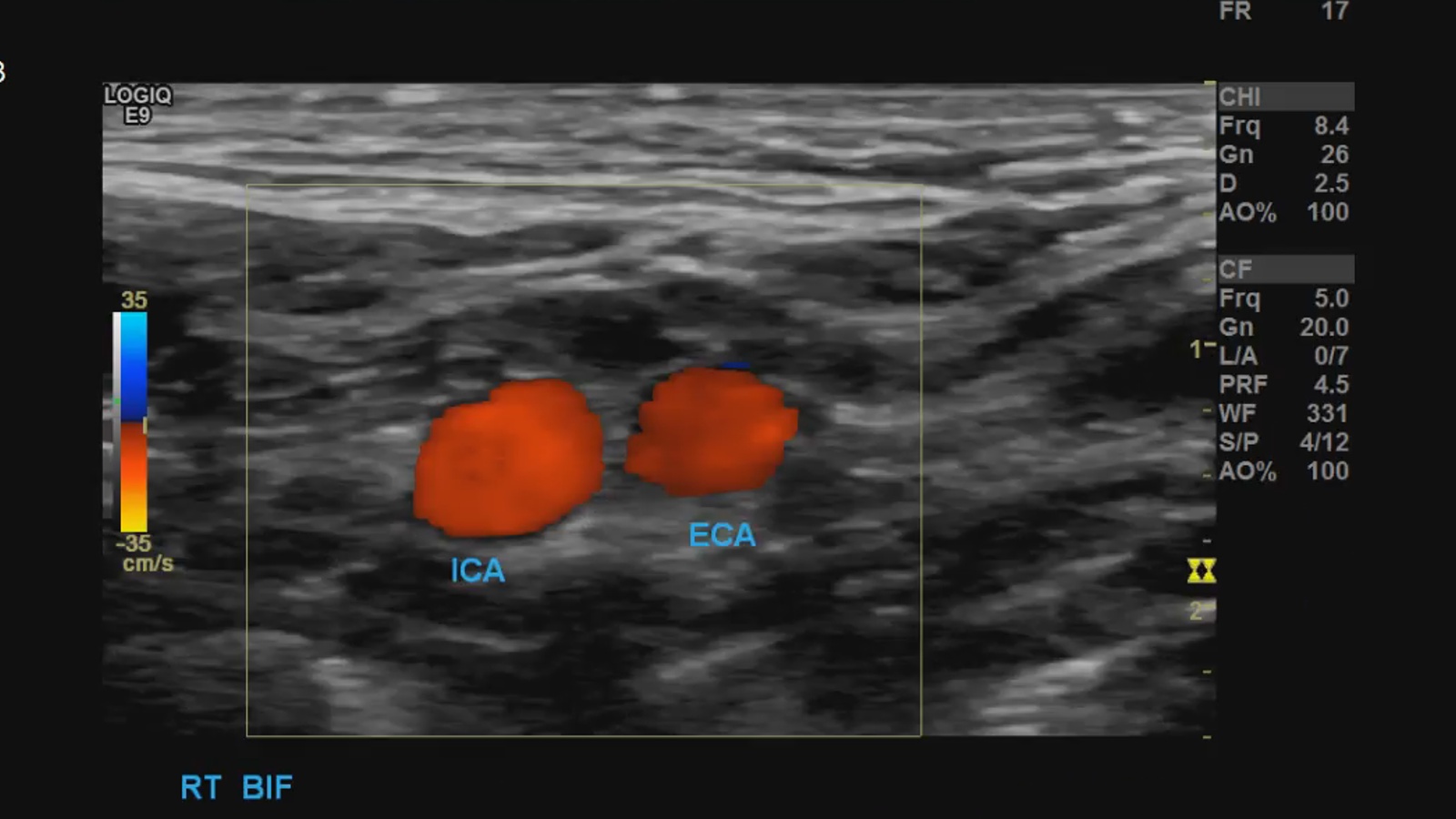
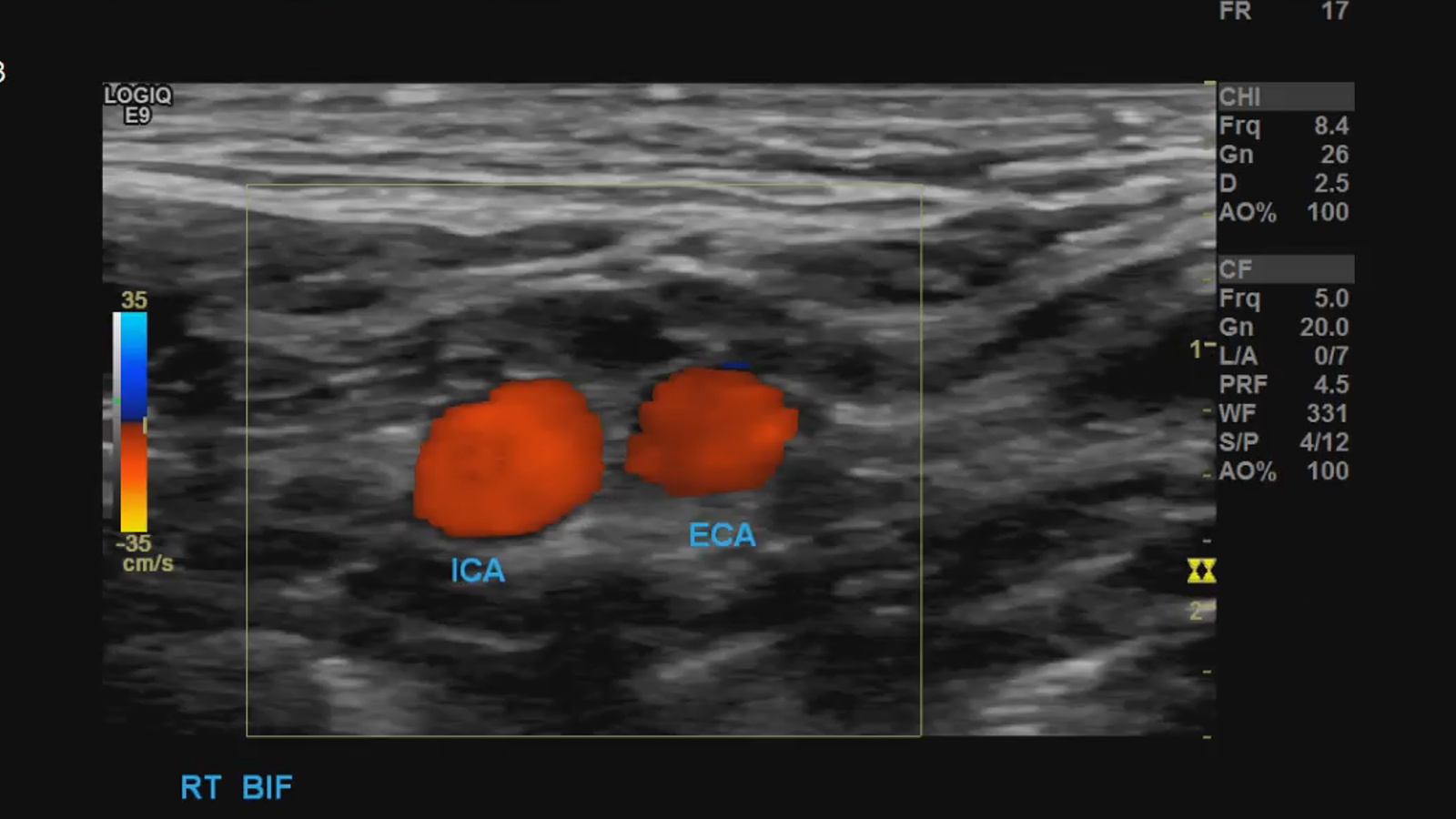
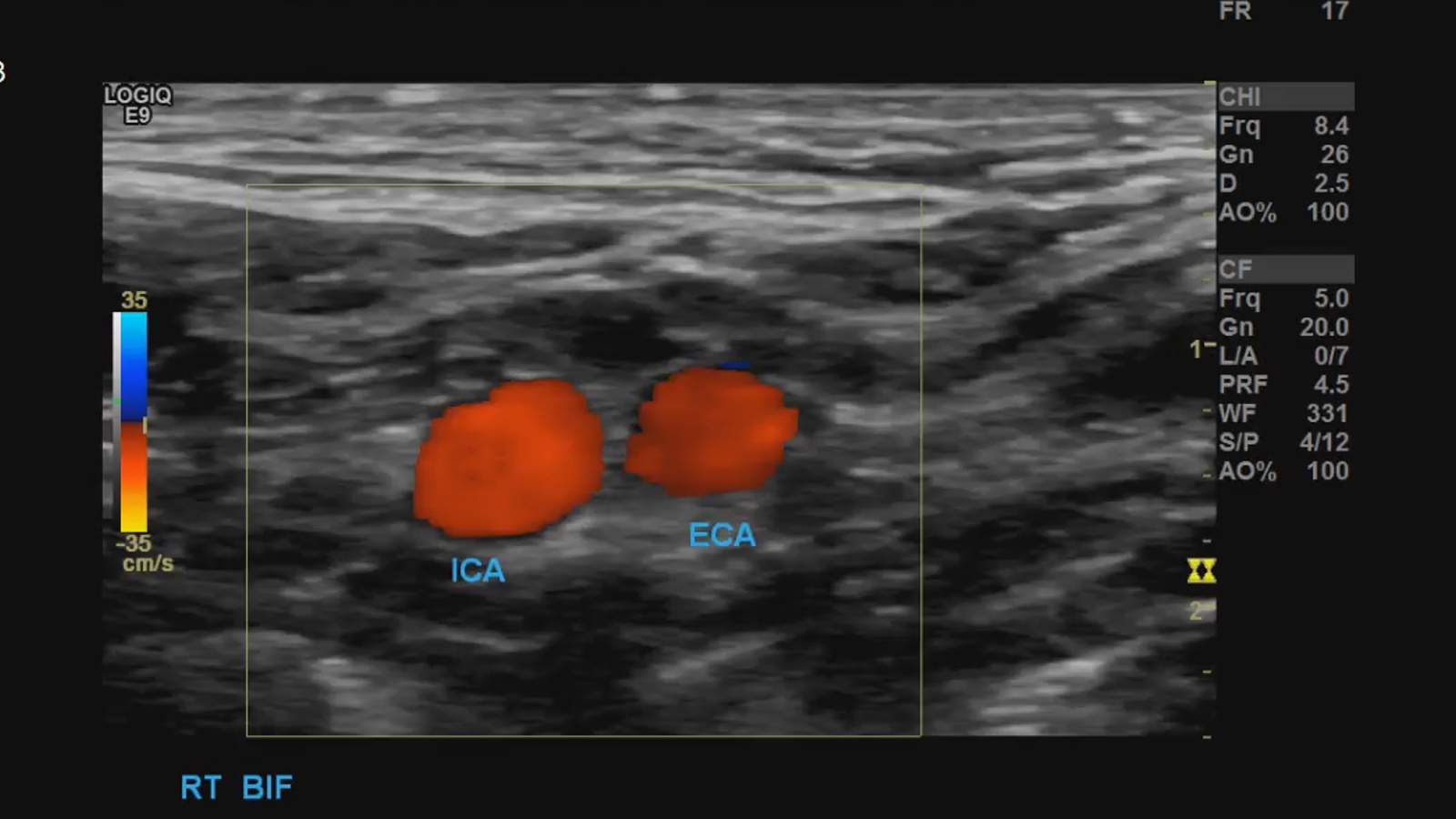
A few tips for differentiating ICA from ECA
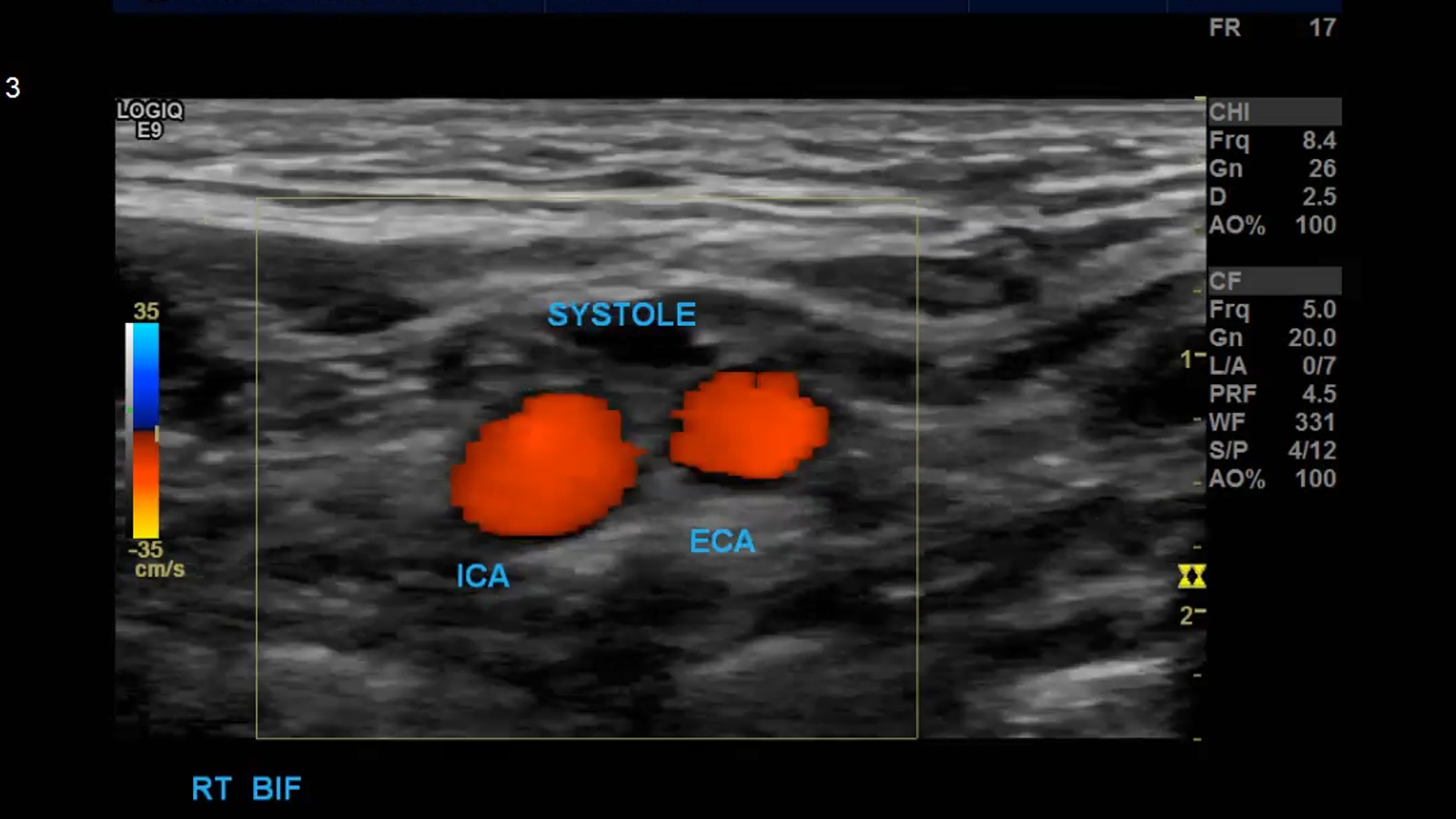
Immediately after the Bulb the ICA is larger in diameter

The ECA has early branches, the ICA does not
Usually the ICA is away from the face, the ECA towards
The waveforms
Transverse color doppler shows “on and off” pattern for ECA and continouous flow for ICA
(Higher resistance in the ECA can mean reduced or no flow in diastole, whereas flow is continuous in the ICA throughout the cardiac cycle)

Temporal Tap
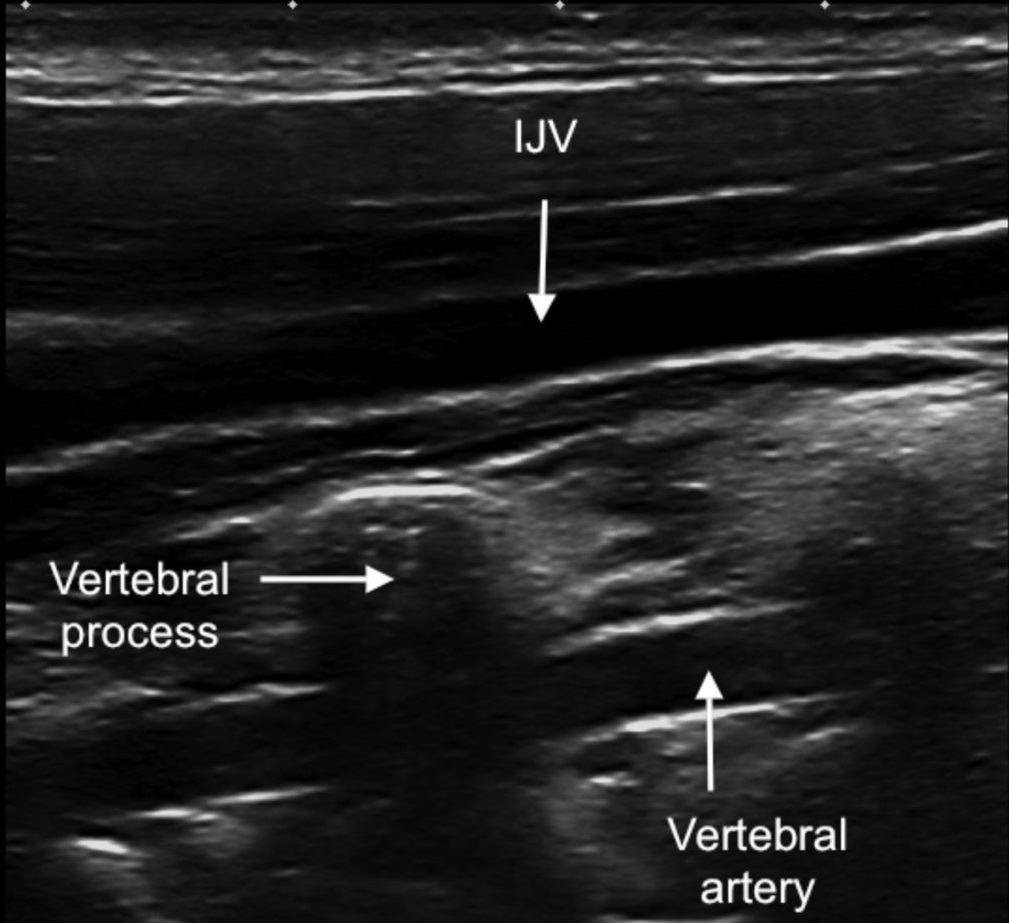
Tips for finding the vertebral artery
- Locate your CCA
- Angle laterally
- Pay attention to direction, use the CCA as a guide, if reversal of flow is seen further imaging to evaluate for Subclavian steal syndrome is necessary.
- If very difficult use a vector probe and scan posteriorly to find the vertebrobasilar confluence
Pathology
Plaque
“Atherosclerosis, or hardening of the arteries, is a condition in which plaque builds up inside the arteries. Plaque is made of cholesterol, fatty substances, cellular waste products, calcium and fibrin (a clotting material in the blood)”. [5]
Appearance can categorize plaques by
Surface
- Smooth
- Irregular
Texture
- Homogenous
- Heterogenous
- Intraplaque hemorrhage and ulceration
Stenosis
If atherosclerotic plaque becomes large enough it can lead to stenosis and blockage. Stenosis can be assessed by color and spectral Doppler.
- Spectral Doppler will show increased velocity, waveforms changes like turbulence, spectral broadening, tardus parvus waveforms post stenotically
- Color Doppler will show aliasing at the site of stenosis (color mosaic pattern), trickle or absent flow in cases of severe, near and complete occlusion
- Stenosis > 60% typically don’t show any significant velocity increases, though waveform changes may be present.
Society of Radiologists in Ultrasound Stenosis Criteria [6]
- https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm3
- http://s0www.utdlab.com/contents/image.do?imageKey=SURG%2F54048
- http://anatomyzone.com/anatomy-feed/transverse-foramen/
- http://www.aium.org/resources/guidelines/extracranial.pdf
- http://www.heart.org/HEARTORG/Conditions/Cholesterol/WhyCholesterolMatters/Atherosclerosis_UCM_305564_Article.jsp#.WIgJIhsrKM8
- http://www.trojanimaging.com/carotid.html
