

Henry Suarez RDMS (AB, OB/GYN, PS) RVT
Gynecomastia
Gynecomastia is benign proliferation of ductal epithelium in the retroareolar region in men, believed to have been first introduced in the second century A.D. The phrase gynecomastia (also spelled gynaecomastia); “gyne” (Greek, γυνή/gyne which means woman or female) and “mastos” (Greek mastos “woman’s breast,”). The first mention of gynecomastia in modern literature is 1902. [1]
The condition itself is self limiting, however patients afflicted with gynecomastia can suffer emotional distress and be unhappy with the cosmetic appearance potentially causing significant negative impact on one’s self-esteem [2], thus treatment may be implemented to reduce these unwanted effects. The cause typically is a result from hormonal imbalance between estrogen and testosterone. Other causes have been linked to; cirrhosis, hypogonadism, renal insufficiency, [3] Grave’s disease, [4] Klinfelters syndrome [5] Gynecomastia can also be seen in trasgender male to female patients receiving exogenous estrogen. [6] Cases of gynecomastia usually resolve on their own without need for further treatment.
Epidemiology and Risk Factors
Gynecomastia is quite prevalent with approximately up 70% of prepubertal males developing the condition. [7] 60% to 90% in neonates, 50% to 60% in adolescents, and up to 70% in men aged 50 to 69 years. [8] Alcohol and certain drug use is a potential risk factor to develop gynecomastia. Phytoestrogens in alcohol and the direct inhibition of testosterone production by ethanol further disrupt the estrogen-to-testosterone ratio.[9] The drugs spironolactone, cimetidine, ketoconazole, hGH, estrogens, hCG, anti-androgens, GnRH analogs and 5-α reductase inhibitors have an association with the development of gynecomastia. [10]
Causes
There are several physiologic and nonphysiologic causes of gynecomastia.
Physiological gynecomastia as well as idiopathic are the most common. [9] Medication or substance abuse as mentioned in the previous paragraph. Primary hypogonadism (5α-reductase deficiency, congenital anorchia, hemochromatosis, klinefelter syndrome to name a few). Some tumors have been associated with gynecomastia including adrenal, gastric carcinoma, large cell lung cancer, pituitary and testicular tumors (particularly Leydig and Sertoli cell tumors). [9]
Radiological Appearance
Imaging findings of gynecomastia are well described with mammography and sonography being very useful in the diagnosis and follow up of this condition.
Mammography
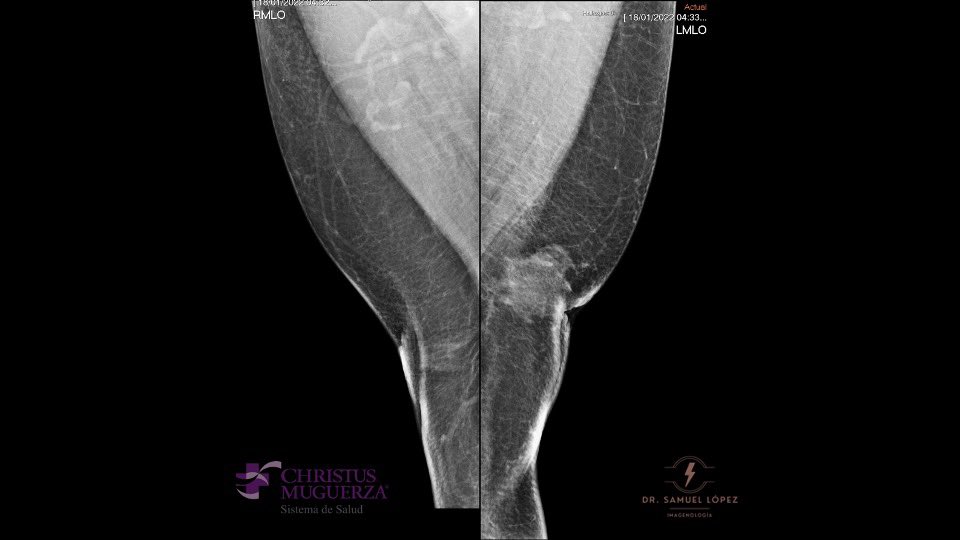
The standard mammographic views are craniocaudal, mediolateral oblique of each breast [11] There are three characteristic patterns of gynecomastia seen at mammography which are nodular, dendritic, and diffuse glandular. [12]
The nodular pattern of gynecomastia (early, florid phase) is indicative of the presence of gynecomastia less than 1 year. Mammography will detect a nodular subareolar density. [12]
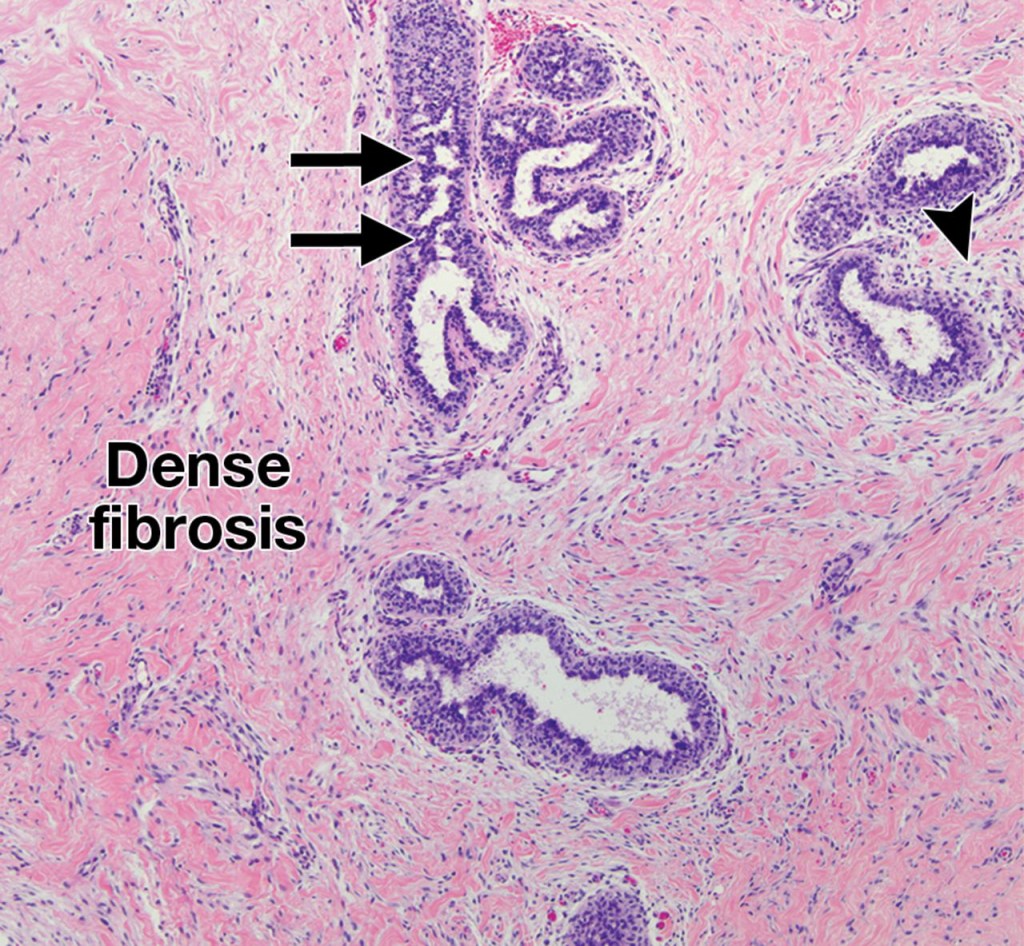
Dendritic gynecomastia (quiescent fibrotic phase) is seen in patients with gynecomastia for longer than 1 year. Histologically there will be stromal fibrosis and dilated ducts. Usually these tissue changes are irreversible. Mammograms of this phase typically show a triangular flame-shaped subareolar density with prominent linear projections permeating the surrounding tissue toward the upper-outer quadrant.[12]
Glandular gynecomastia can be seen in patients taking exogenous estrogen. Mammography will reveal enlargement of the breast and diffuse density with both dendritic and nodular features. [12]
Ultrasound
On ultrasound gynecomastia often appears as a retroareolar, triangular, hypoechoic ~80% mass that can be unilateral or bilateral. [14,15] This represents glandular tissue, there may also be dilated ducts and increased adipose tissue.



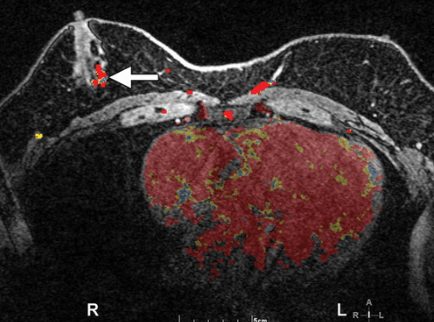
Fig. 3 radial and antiradial sonogram of the left nipple-areolar complex showing diffuse, triangular hypoechoic tissue consistent with gynecomastia. Fig. 4 Color doppler and elastography images. Fig. 5 panoramic views of the right and left breast showing left gynecomastia (red arrow) (Dr. Samuel Lopez used with permission)

CT
Computed tomography is not routinely used to evaluate for gynecomastia, However gynecomastia is found routinely on CT of the chest done for other clinical indications. In one review, a clinical sample of 25.6% of patients showed gynecomastia on CT imaging (21 of 82 patients). [17]
MRI
MRI is also not routinely used in the surveillance of gynecomastia, this case demonstrates the MRI appearance of a nodular bilateral asymmetric gynecomastia. [12]
Diagnosis
Diagnosis of gynecomastia is often made with a complete physical and seldom requires further imaging or work up. In cases where imaging is used ultrasound as well as mammography is often utilized. Patients with gynecomastia often present with breast pain and/or palpable mass (unilateral or bilateral). In other occurrences, gynecomastia is found on routine physical examination. A detailed history is routinely taken to rule out other causes of gynecomastia. Symptoms longer than two years suggest a non-physiological cause of gynecomastia. [ 9] Physical examination include palpation of the male breast tissue. Evaluation of male genitalia for development and testicels for masses that may indicate testicular cancer. Fine-needle aspiration is often not used and should only be implemented in cases of suspected malignancy. Males with Klinefelter syndrome appear to have a risk of developing breast cancer 16 to 30 times higher than men without the condition. [9]
Differential Diagnosis
- Mastitis
- Breast cancer
- Pseudogynecomastia (excess adipose tissue mimicking gynecomastia)
- Lipoma
- Sebaceous cyst
- Dermoid cyst
- Hematoma
- Metastasis [9]
Treatment
Patients with gynecomastia typically do not require treatment aside from analgesia for pain. Cases where the cosmetic impact of gynecomastia require some form of plastic surgery are not common. [18] Several drugs in the SERM family (Selective estrogen receptor modulators) have been shown to potentially be effective in the treatment of gynecomastia however there is no Food and Drug Administration (FDA) approval for uses of these drugs in gynecomastia.
Surgery
In cases of persistent disease, surgery may be utilized to remove the glandular tissue. In cases of pseudogynecomastia no treatment is needed and the patient can be counseled on the efficacy of exercise, diet and weight loss in the resolution of pseudogynecomastia. [9]
Prognosis
In the absence of underlying causative disease (i.e Klinfelter syndrome, hormone releasing tumor) gynecomastia is self limiting and does not pose any physical threat to the patient. Patients may have secondary psychological/self esteem difficulties that should be addressed.
Conclusion
Gynecomastia is the most common breast condition in males. This condition is easily diagnosed on physical examination and can be further evaluated with imaging in some cases. Gynecomastia is self limiting and usually goes away on its own. Persistent gynecomastia should raise concern of underlying condition and requires further work up. In a small percentage of cases gynecomastia can have a negative effect on self esteem and emotional well being and plastic surgery is an option to treat the conditions physical manifestation.
Bibliography
- Bird R. Cases of Gynæcomastia. Ind Med Gaz. 1902 Jan;37(1):19-20. PMID: 29003680; PMCID: PMC5156221.
- Guss CE, Divasta AD. Adolescent Gynecomastia. Pediatr Endocrinol Rev. 2017 Jun;14(4):371-377. doi: 10.17458/per.vol14.2017.GD.Gynecomastia. PMID: 28613047.
- Dickson G. Gynecomastia. Am Fam Physician. 2012 Apr 1;85(7):716-22. PMID: 22534349.
- Sakulterdkiat T, Romphothong K, Chatchomchuan W, Nakasatien S, Krittiyawong S, Thewjitcharoen Y, Himathongkam T. Unilateral gynecomastia as an initial presentation of hyperthyroid Graves’ disease. Endocrinol Diabetes Metab Case Rep. 2021 Nov 1;2021:20-0140. doi: 10.1530/EDM-20-0140. Epub ahead of print. PMID: 34747364; PMCID: PMC8630755.
- Kanakis GA, Nieschlag E. Klinefelter syndrome: more than hypogonadism. Metabolism. 2018 Sep;86:135-144. doi: 10.1016/j.metabol.2017.09.017. Epub 2018 Jan 31. PMID: 29382506.
- Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E. & Mulder, J. W. Short-term and long-term histologic effects of castration and estrogen treatment on breast tissue of 14 male-to-female transsexuals in comparison with two chemically castrated men. Am. J. Surg. Pathol. 24, 74–80 (2000).
- NYDICK M, BUSTOS J, DALE JH Jr, RAWSON RW. Gynecomastia in adolescent boys. JAMA. 1961 Nov 4;178:449-54. doi: 10.1001/jama.1961.03040440001001. PMID: 14480779.
- Johnson, R. E., & Murad, M. H. (2009). Gynecomastia: pathophysiology, evaluation, and management. Mayo Clinic proceedings, 84(11), 1010–1015. https://doi.org/10.1016/S0025-6196(11)60671-X
- GRETCHEN DICKSON, MD, MBA, University of Kansas School of Medicine, Wichita, Kansas Am Fam Physician. 2012 Apr 1;85(7):716-722.
- Deepinder F, Braunstein GD. Drug-induced gynecomastia: an evidence-based review. Expert Opin Drug Saf. 2012 Sep;11(5):779-95. doi: 10.1517/14740338.2012.712109. Epub 2012 Aug 6. PMID: 22862307.
- .P K Chantra, G J So, J S Wollman, and L W Bassett Mammography of the male breast
American Journal of Roentgenology 1995 164:4, 853-858
- Cheri Nguyen , Mark D. Kettler, Michael E. Swirsky, Vivian I. Miller, Caleb Scott, Rhett Krause, Jennifer A. Hadro. “Male Breast Disease: Pictorial Review with Radiologic-Pathologic Correlation.” RadioGraphics, 3 May 2013, pubs.rsna.org/doi/10.1148/rg.333125137.
- Chen L, Chantra PK, Larsen LHet al.. Imaging characteristics of malignant lesions of the male breast. RadioGraphics 2006;26(4):993–1006
- P K Chantra, G J So, J S Wollman and L W Bassett. Mammography of the male breast. AJR April 1995, Volume 164, Number 4
- Vandana Dialani MD,Janet Baum MD,Tejas S. Mehta MD, MPH. Sonographic Features of Gynecomastia First published: 01 April 2010 https://doi.org/10.7863/jum.2010.29.4.539
- Narula, H. S., & Carlson, H. E. (2014). Gynaecomastia—pathophysiology, diagnosis and treatment. Nature Reviews Endocrinology, 10(11), 684–698. doi:10.1038/nrendo.2014.139
- Gossner J. (2018). Gynecomastia on Computed Tomography of The Chest -Prevalence in A Clinical Population and An Analysis of Possible Causes. European journal of breast health, 15(1), 67–68. https://doi.org/10.5152/ejbh.2018.4330
- Hanavadi S, Banerjee D, Monypenny IJ, Mansel RE. The role of tamoxifen in the management of gynaecomastia. Breast. 2006;15(2):276–280.

Points taken
LikeLike