

Hey there everyone, today we’re going to go on sonographic journey through diseases reliably discovered via ultrasound.
We will focus only on the kidneys.
The badder as well as renovascular pathology will be covered in the future.
Diseases
- Hydronephrosis
- Echogenic kidneys
- Inflammatory/infectious processes
- Renal cystic disease
- Trauma
- Masses
will not go over developmental anomalies or nephrolithiasis in great detail as I covered them on other blogs/videos.
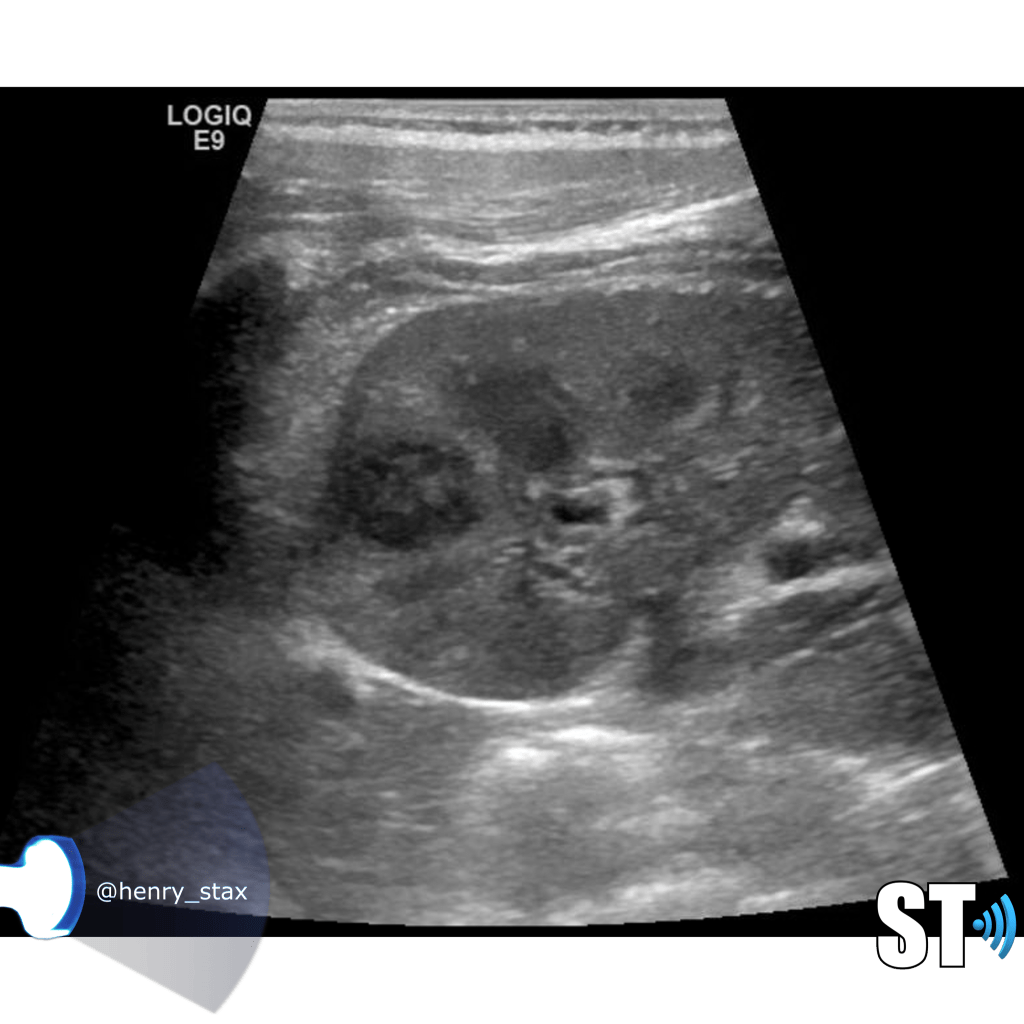
Hydronephrosis
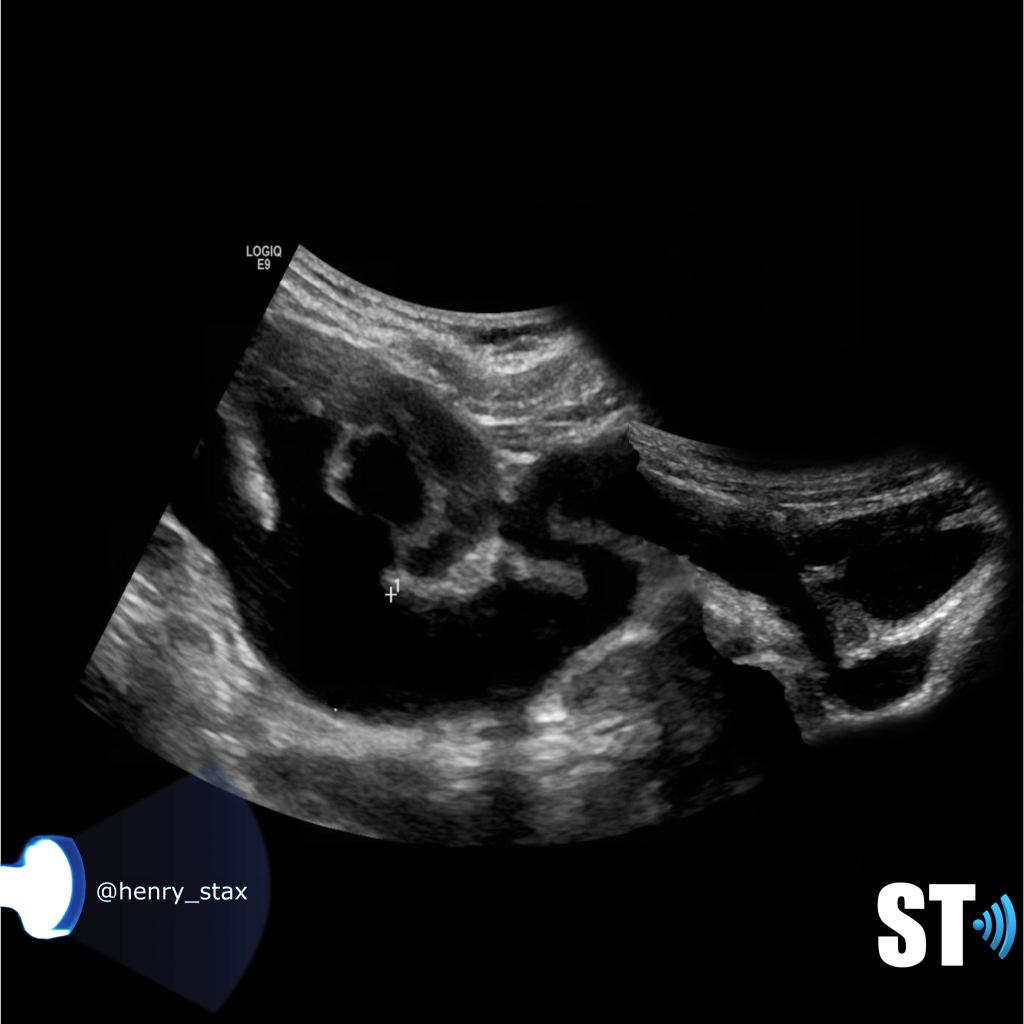
Now for starters hydronephrosis is not a disease, it is a plumbing issue due to some underlying disease. Whether it be a tumor in the abdomen pressing on the bladder, a sneaky stone stuck in either end of the ureter, or the middle for that matter. Or some developmental anomaly causing kinked or blocked ureters.
Our job is to detect the blockage we call hydronephrosis, we may even be helpful in offering a possible cause.
So let’s break down hydro into obstructive and nonobstructive causes.
Obstructive
- Stones
- UPJ and UVJ obstructions
- Urethral valves
- Masses
- Prostatic (hyperplasia/tumors)
Non obstructive
- Vesicoureteral reflux
- Megaureter
- Pyelonephritis

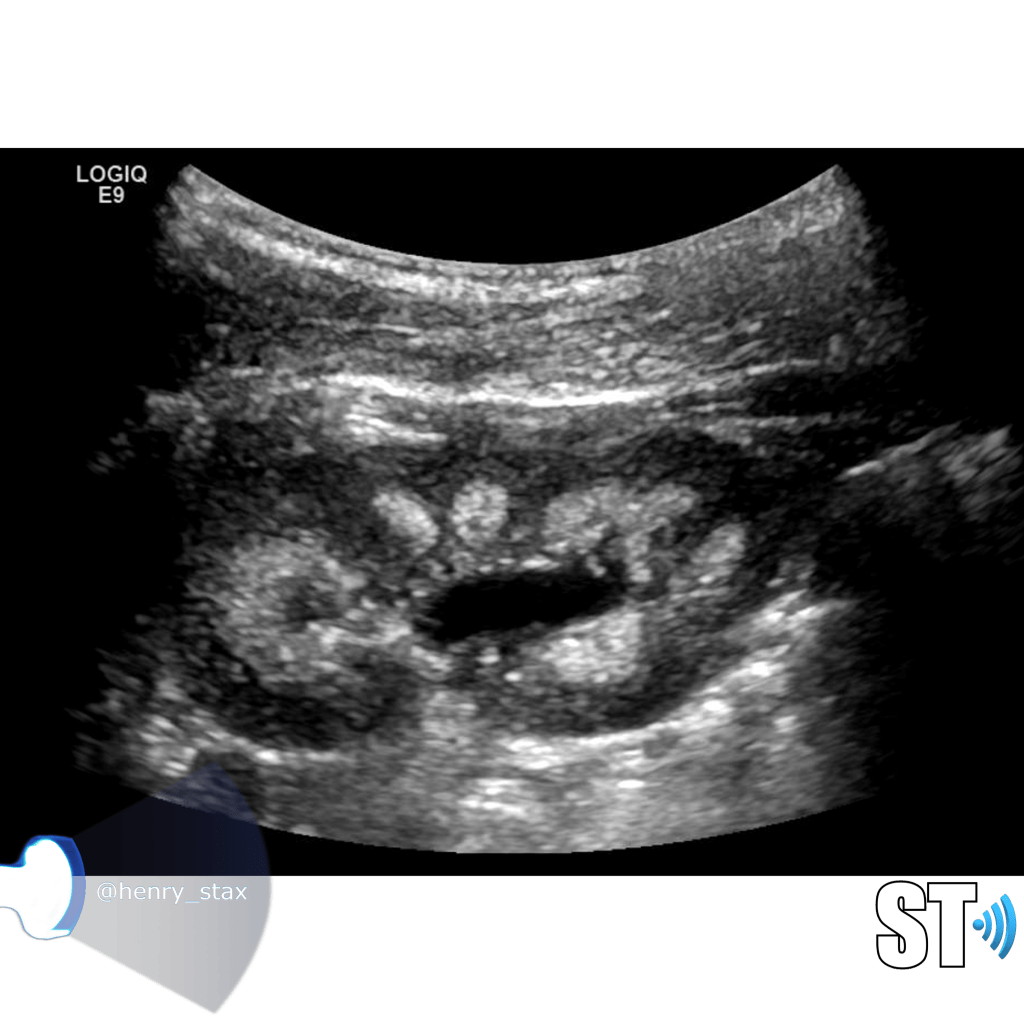
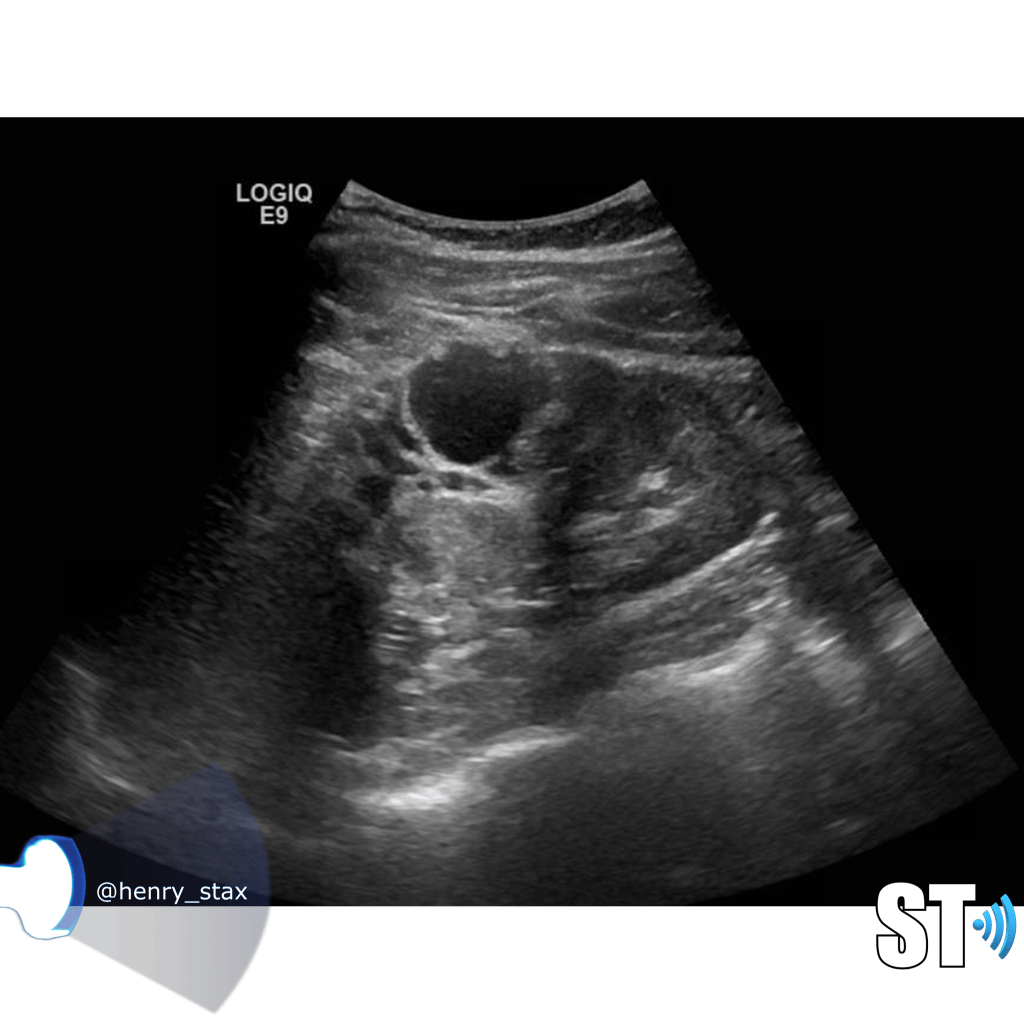
A simple way to grade hydronephrosis is by severity, mild to severe.
Mild
Pelvic fullness with no calyceal dilatation
Moderate
Greater expansion of the renal pelvis and involvement of the calyces
Severe
Further dilatation of the renal collecting system with cortical thinning
It’s good practice to always place color doppler on mild hydronephrosis or extra-renal pelves to distinguish a true fluid collection form a prominent renal vein.
Reflux Nephropathy
Reflux nephropathy is damage to kidney caused by vesicoureteral reflux. The affected kidneys can have focal areas of cortical thinning, or can be completely atrophic depending on the lenght and degree of disease.




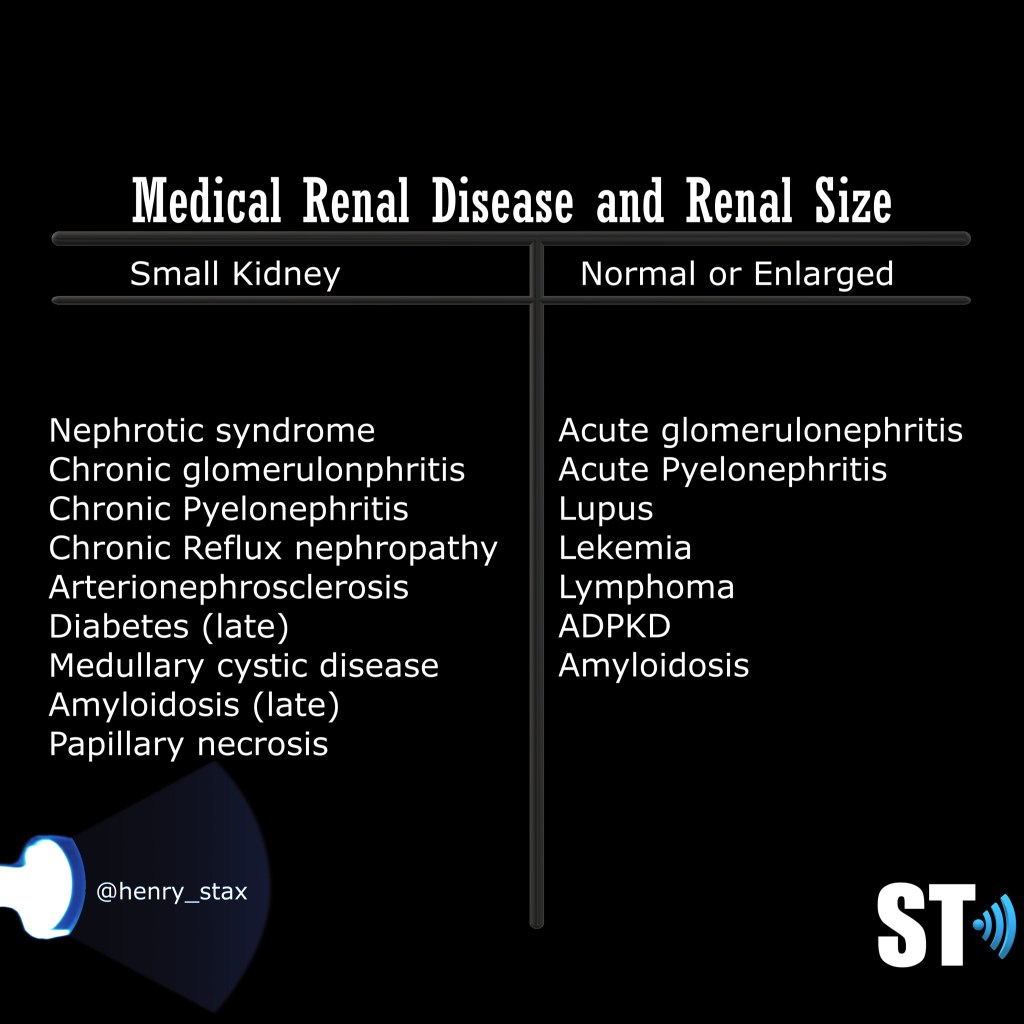
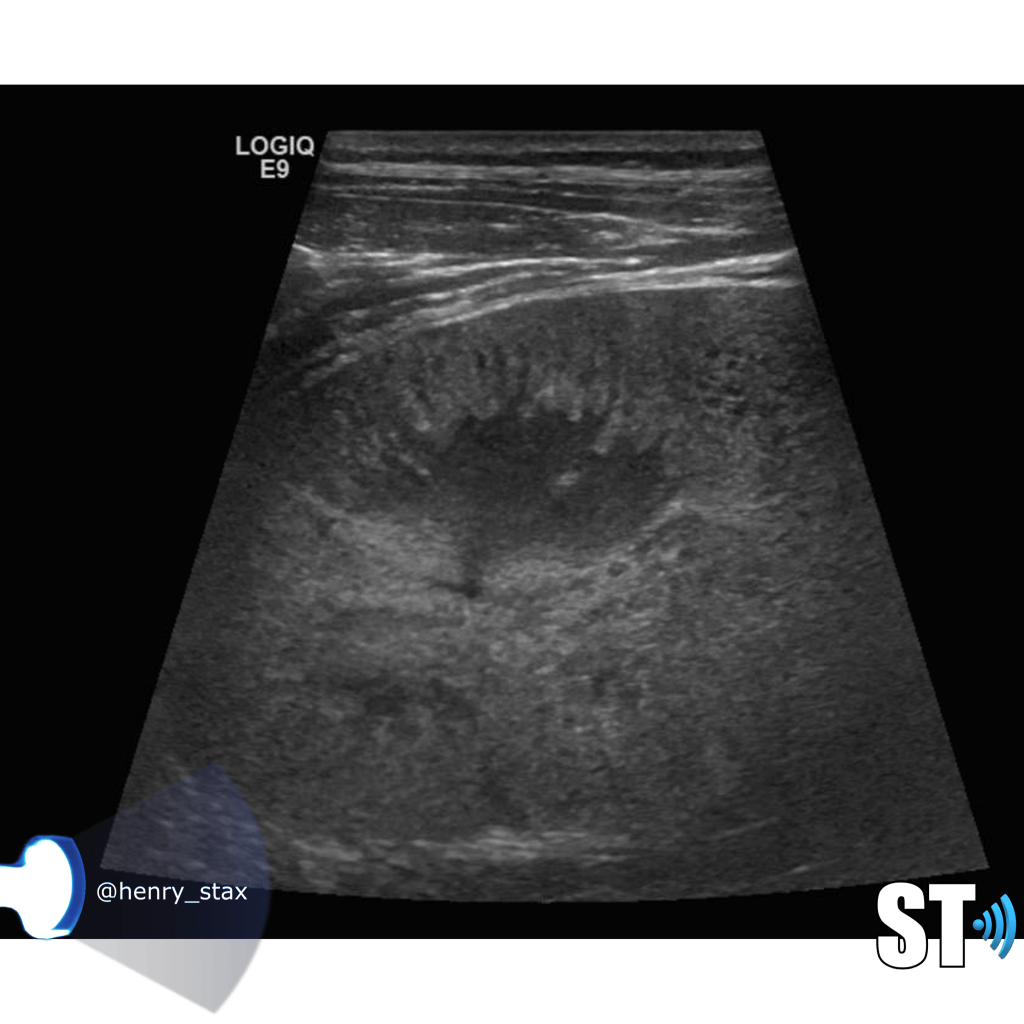
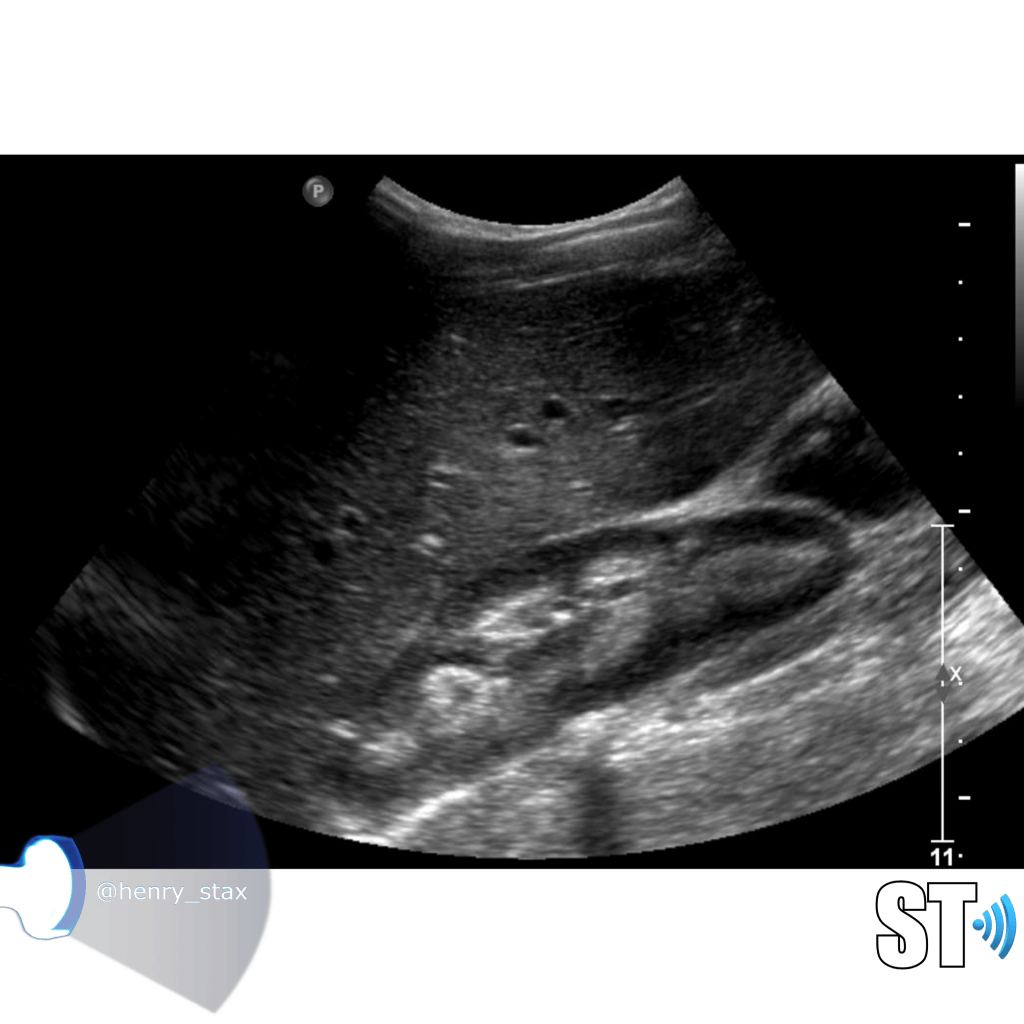
Renal Echogenicity
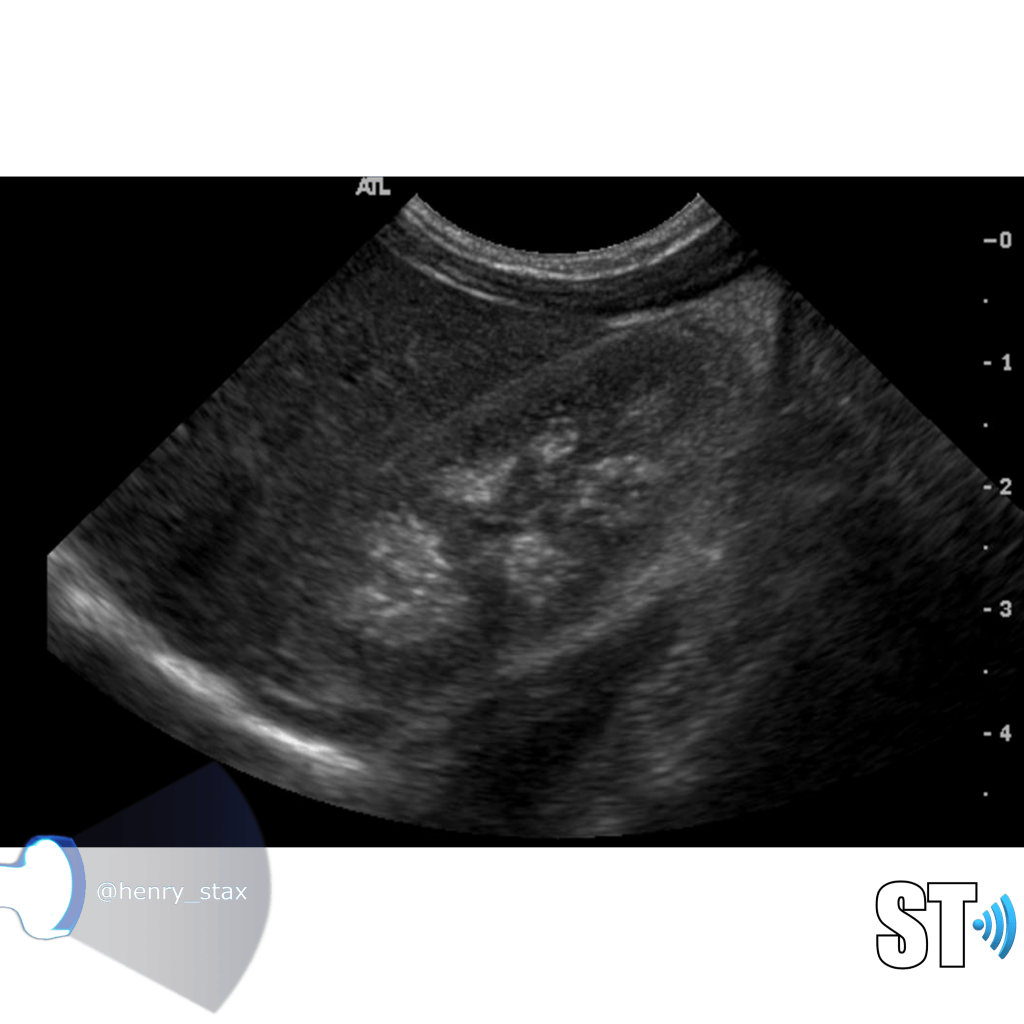
Another ultrasound sign of disease is echogenicity. Increased echogenicity is when the parenchymal echoes are greater than the liver. Usually the kidney is hypoechoic to almost isoechoic to the liver. Many different entities can cause increased echogenicity, that’s why when a radiologist reads an ultrasound with hyperechoic kidneys they usually attribute it to “medical renal disease”. A very hypoechoic kidney is also not normal, especially when it is focal as this could be due to infarction or infection.
The echogenicity of the kidney is just a single data point along with clinical and other laboratory findings a clinician can use in diagnosing renal disease.
For our purposes we need to tell whether the kidneys are hyperechoic or not, also is the corticomedullary (cmd) differentiation preserved or is it lost, this can give you clues as to the chronicity of renal parenchymal disease. If the cmd is easily seen it may suggest a more acute process, whereas chronic disease will usually show echogenic and atrophic kidney with little to no differentiation of the cortex to medulla


Infection
UTI’s are very common, presenting symptoms are urinary frequency, painful urination and hematuria. They’re more common in women for anatomical reasons.
Many times you’ll get an ultrasound ordered for UTI in babies from the ER. For recurrent UTIs or really young patients they’re gonna be referred for an outpatient renal and VCUG combo to look for reflux as a causal factor…
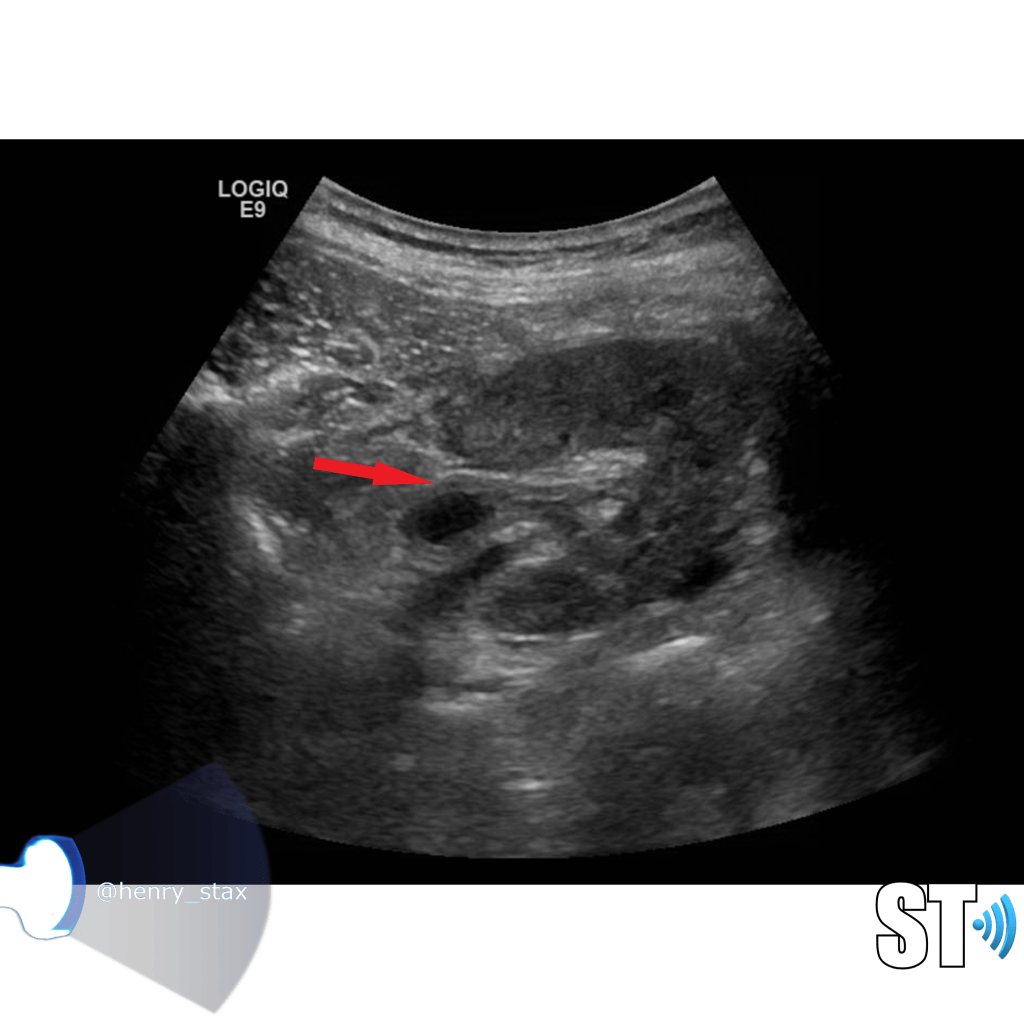
As a UTI ascends you may see cystitis or bladder inflammation. Typically bladder wall thickening with hyperemia, and bladder debris, though debris is sometimes seen in patients without UTI.
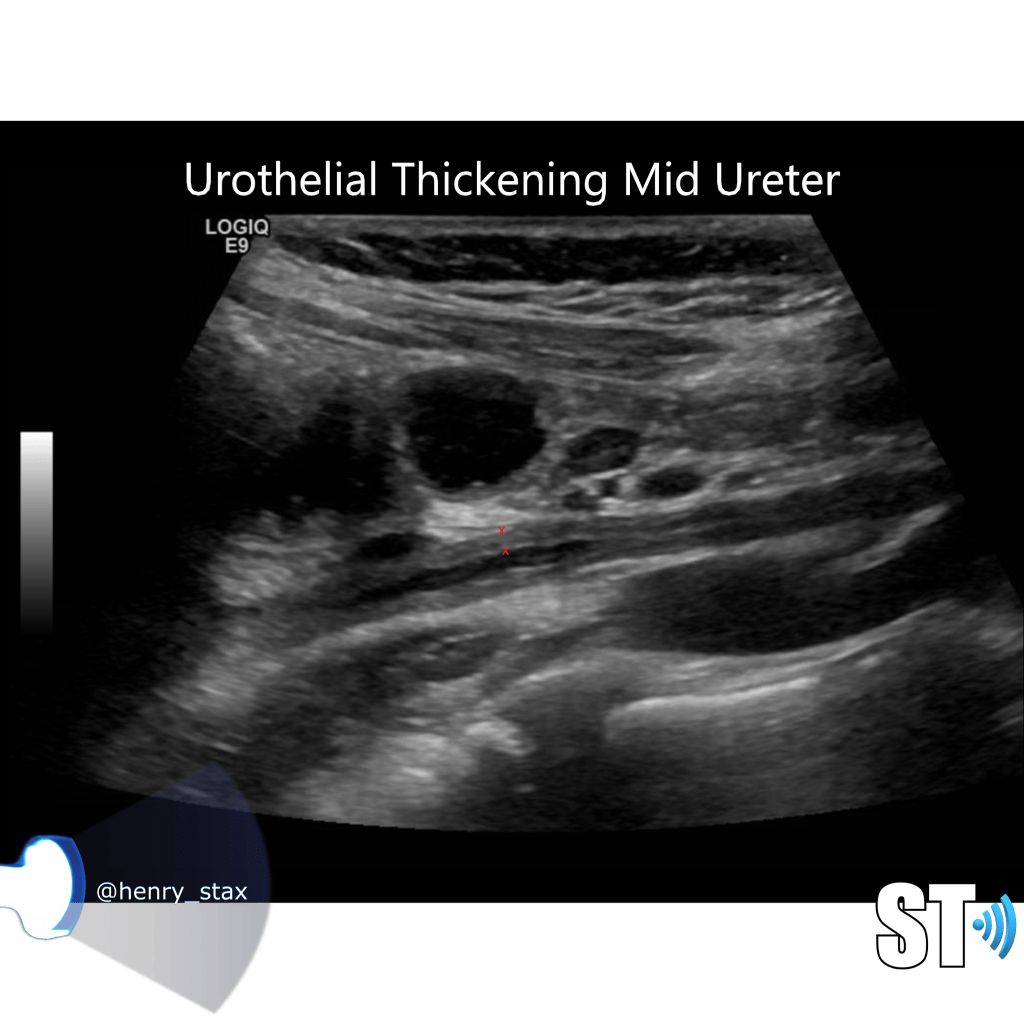
Further up you may see thickening of the ureteral urothelium, obviously this is more apparent in thin patients and pediatrics.
Urothelial thickening can also be seen in the renal pelvis.
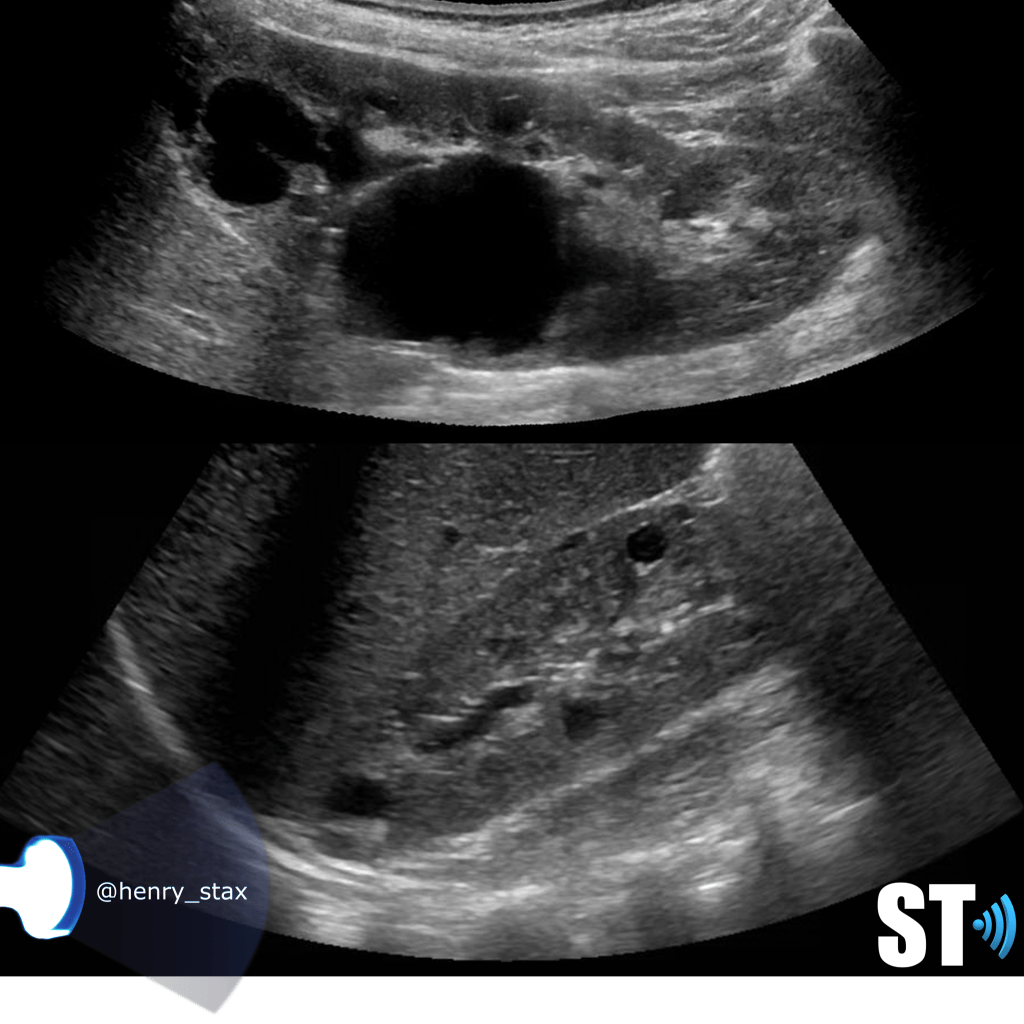
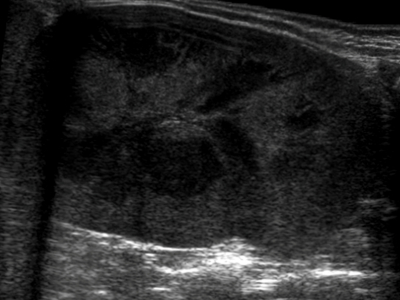
Acute pyelonephritis
Bacterial inflammatory disease of the kidney is commonly cause Eschericia coli. Most infections begin as UTI that ascends to the upper genitourinary system. the infection spreads from the renal pyramids into the renal cortex. The infection may be focal or diffuse. This condition usually presents with chills, fever, flank pain and laboratory findings of urinary infection.
Ultrasound may show an enlarged kidney with edema and increased echogenicity. You may also see a focal triangular area of altered echogenicity that displays reduced perfusion with color Doppler and power Doppler. If left untreated or inadequately treated that area can turn into an abscess.
An abscess will be well formed and distinct from the remainder of the renal parenchyma, it will be heterogeneous, complex appearance with mixed echoic and anechoic portions and no color doppler signal internally..
Once an abscess has formed drainage under ultrasound guidance can be performed. On subsequent imaging you notice some cortical thinning where the abscess was representing scarring.
Chronic Pyelonephritis
Chronic pyelonephritis can present as a focal scar from a healed pyelnophritis in the form of focal cortical thinning, If the inflammatory process is diffuse the kidney will be atrophic and scarred.

Glomerulonephritis
Glomerulonephritis is a collection of conditions that affect the glomerulus of the kidney as a result of immunological reactions involving the capillaries of the glomeruli. The kidney reacts to this immune response by
- Cellular proliferation
- Leukocytic infiltration
- Thickening of the glomerular basement membrane
- Hyalinization adn sclerosis
Patients typucally present with heamturia, azotemia, hypertension and red cell casts in the urine. Ultrasound findings are nonspecific you may see the range from normal kidneys to enlargement and increased echogenicity. With chronic glomerulonephritis you’ll typically see atrophic echogenic kidneys indistinguishable from kidneys in end stage renal failure.
Types
- Focal segmental glomerulosclerosis
- Membranous glomerulonephritis
- Iga nephropathy
- Post streptococcal glomerulonephritis
- Goodpasture syndrome

Xanthogranulomatous Pyelonephritis
(Xantho – yellow/Granuloma- collection of macrophages)
Rare form of chronic pyelonephritis usually caused by proteus mirabilis or E.coli. It usually occurs in the presence of long term obstruction. The kidney is non functioning, there is typically a calculus involved, usually a staghorn. A mass may be present that can be mistaken for a renal cell carcinoma, the microscopic features are lipid-laden foamy macrophages accompanied by chronic and acute inflammatory cells.



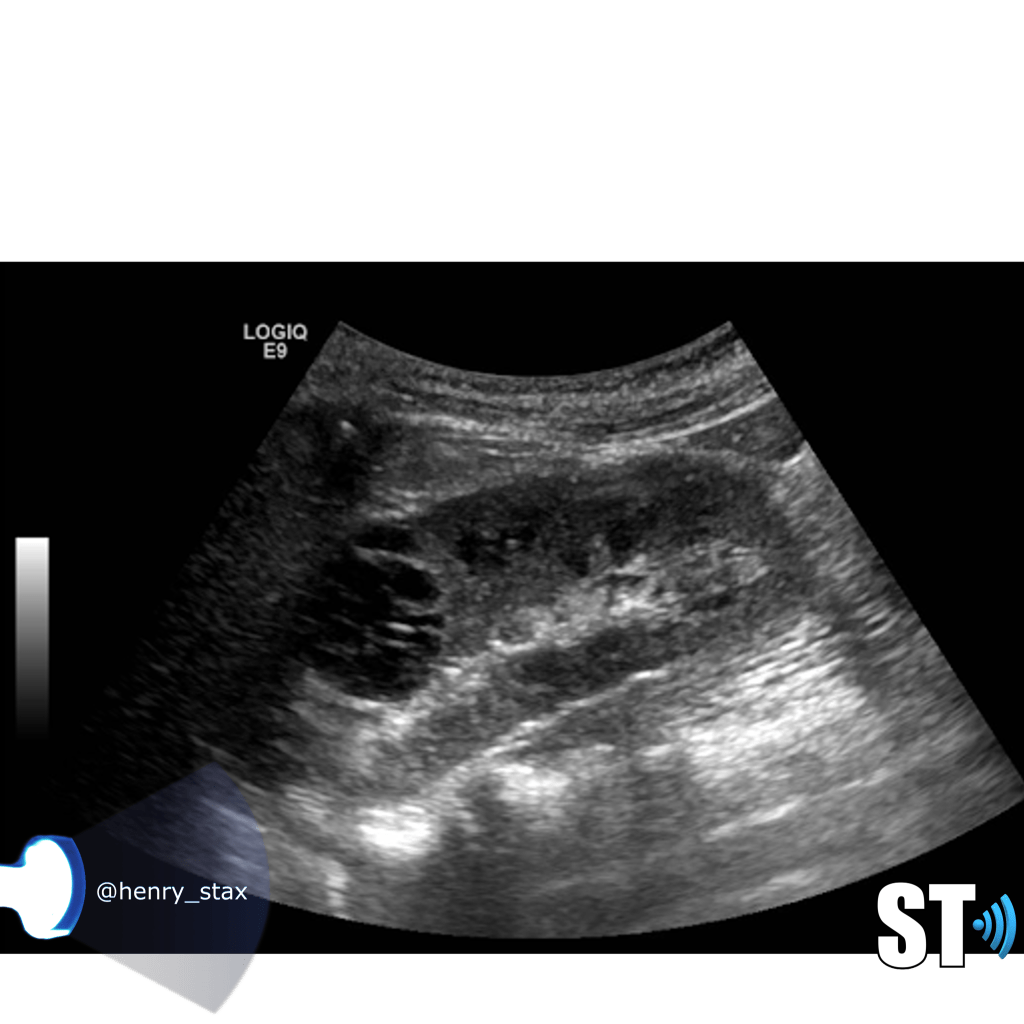
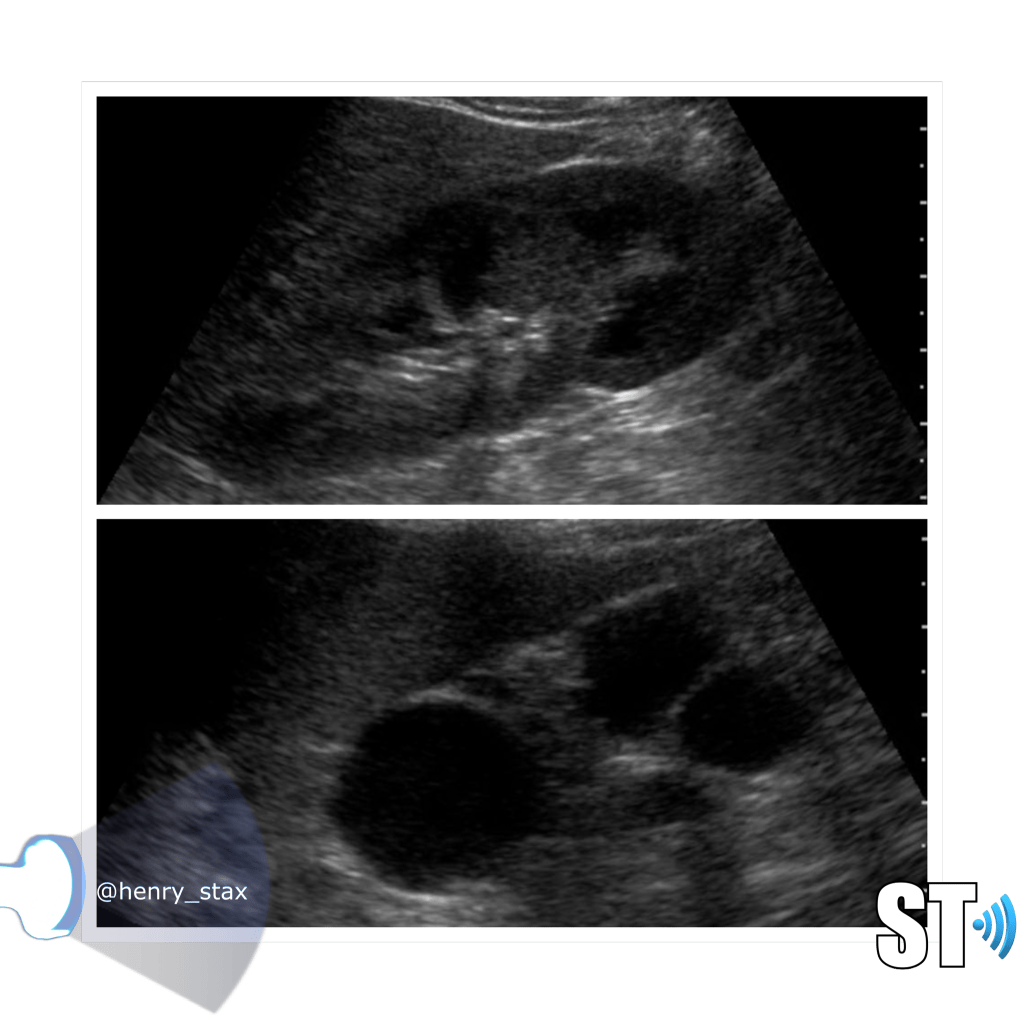
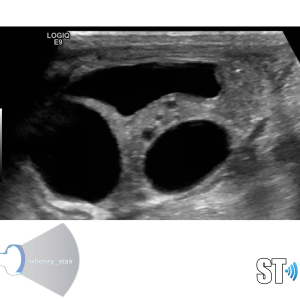
Renal Cystic Disease
Renal cysts are very common and as a sonographer you’ll encounter them frequently in the pediatric and adult populations. Approximately 50% of people who are 50 years and older have simple kidney cysts. The majority of parenchymal cystic lesions are simple epithelial cysts. They have thin walls, are anechoic, good through transmission. They can have thin septations or internal debris(5%) these may require follow up. Chronically some can develop calcifications on their walls.
Types of cystic kidney diseases
- Multicystic dysplastic kidney (MCDK)
- Autosomal recessive polycystic kidney disease (ARPKD),
- Autosomal dominant polycystic kidney disease (ADPKD),
- Medullary cystic kidney disease (MCKD)
- Cysts associated with systemic disease
-Von Hippel-Lindau syndrome
-Tuberous sclerosis
- Acquired – Simple cysts, acquired cystic renal disease, medullary sponge kidney
- Tumors – Cystic renal cell carcinoma, Multilocular cystic nephroma
Simple cysts
Cysts are non functioning parts of the kidney. Simple cysts typically pose no health problems. Simple cysts are often found incidentally when the patient is undergoing a procedure for some other complaint. To meet the criteria for cysts the lesion should be
- Round or oval
- Thin wall
- Anechoic
- Good through transmission (posterior acoustic enhancement)

MCDK
Multicystic Dysplastic Kidney results from a ureteral obstruction before the 8th or 9th week of fetal development. MCDK is usually diagnosed prenatally or shortly after birth if an ultrasound is ordered. The affected kidney is non functioning and is replaced by cysts of various sizes and connective tissue.
- Malformation of the kidney during fetal development
- Multiple cysts
- Contralateral UPJ obstruction is found in 3% to 12%
- Usually unilateral (bilateral form is usually fatal)
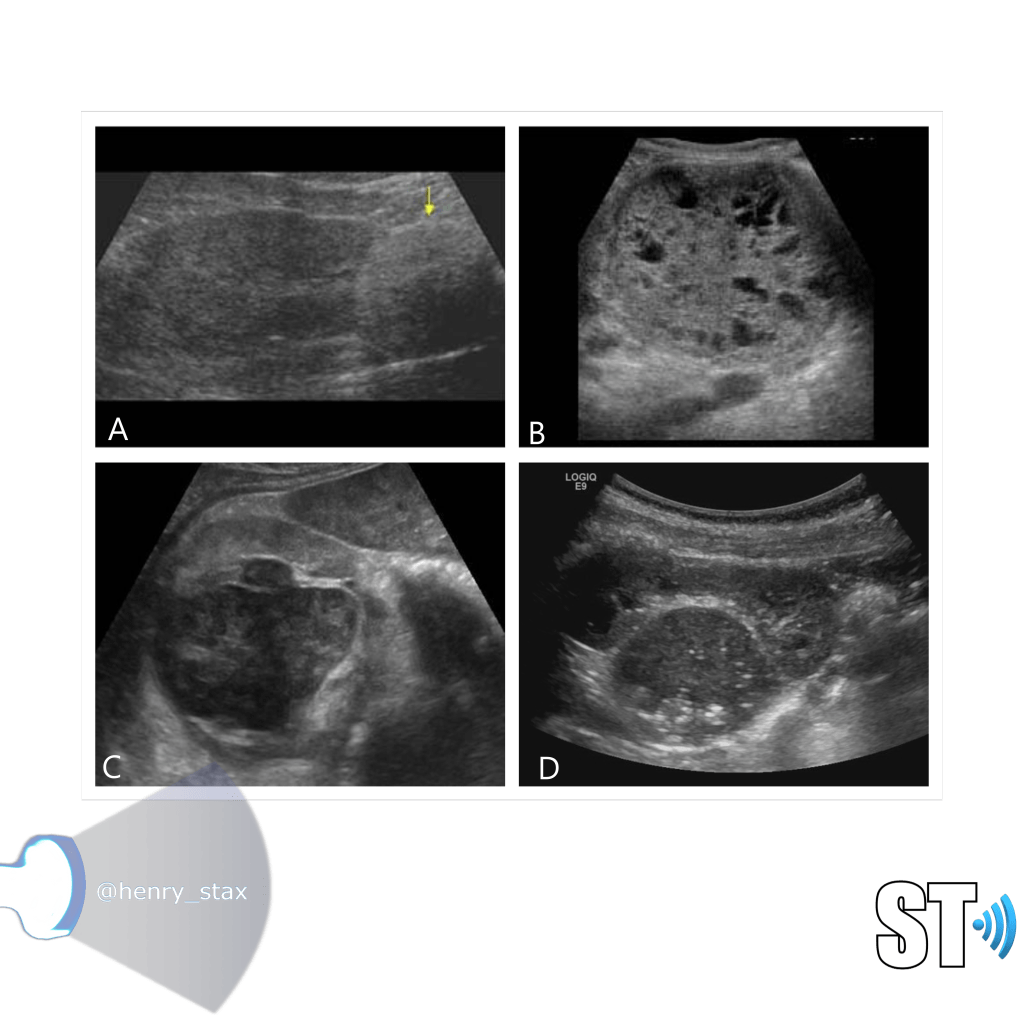
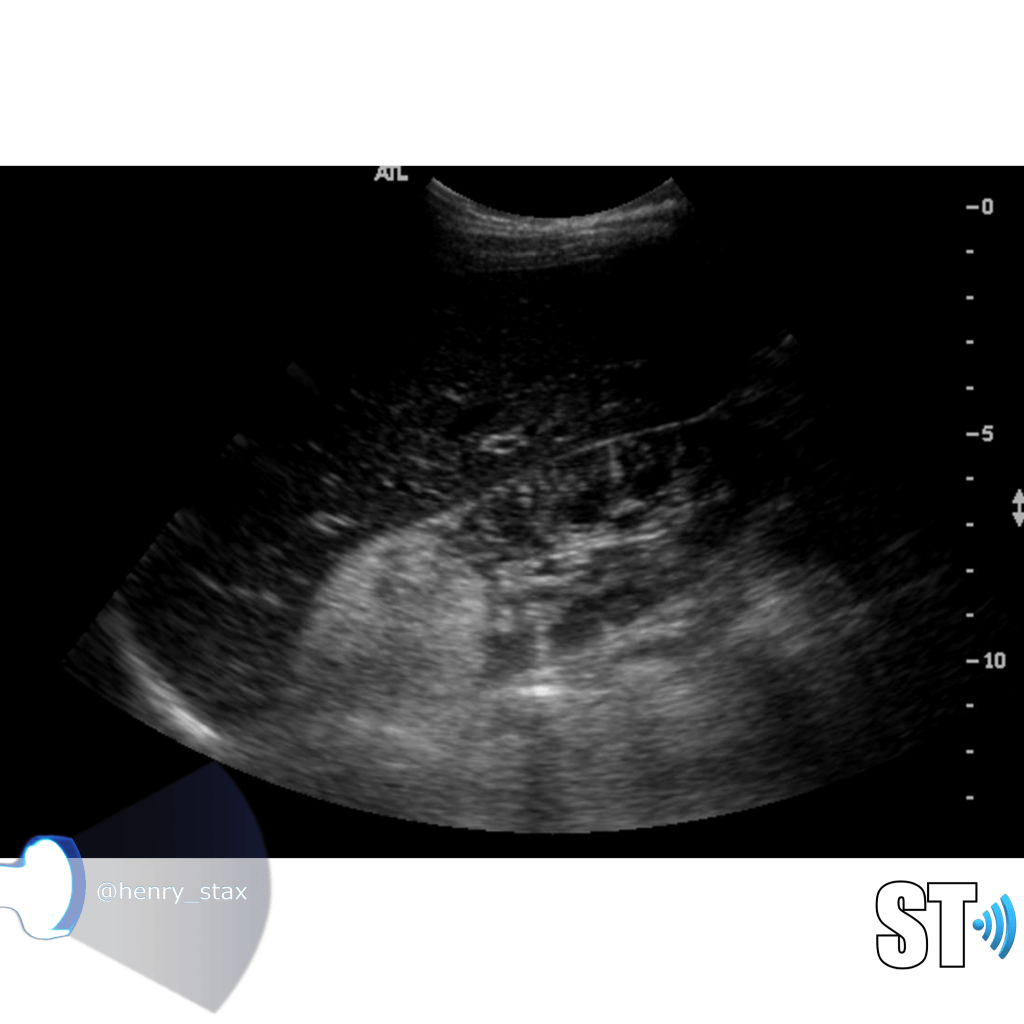
ARPKD
Autosomal Recessive Polycystic Kidney Disease (ARPKD) Typically presents around birth, though it can present later in childhood. Cases that develop later have a propensity to be associated with hepatic fibrosis. ARPKD is transmitted in an autosomal recessive pattern meaning two copies of an abnormal gene must be present in order for the disease or trait to develop.
- Infantile
- Kidney enlargement (sometimes massive)
- >80% liver cysts
- Multiple organs affected
- Hyperechoic

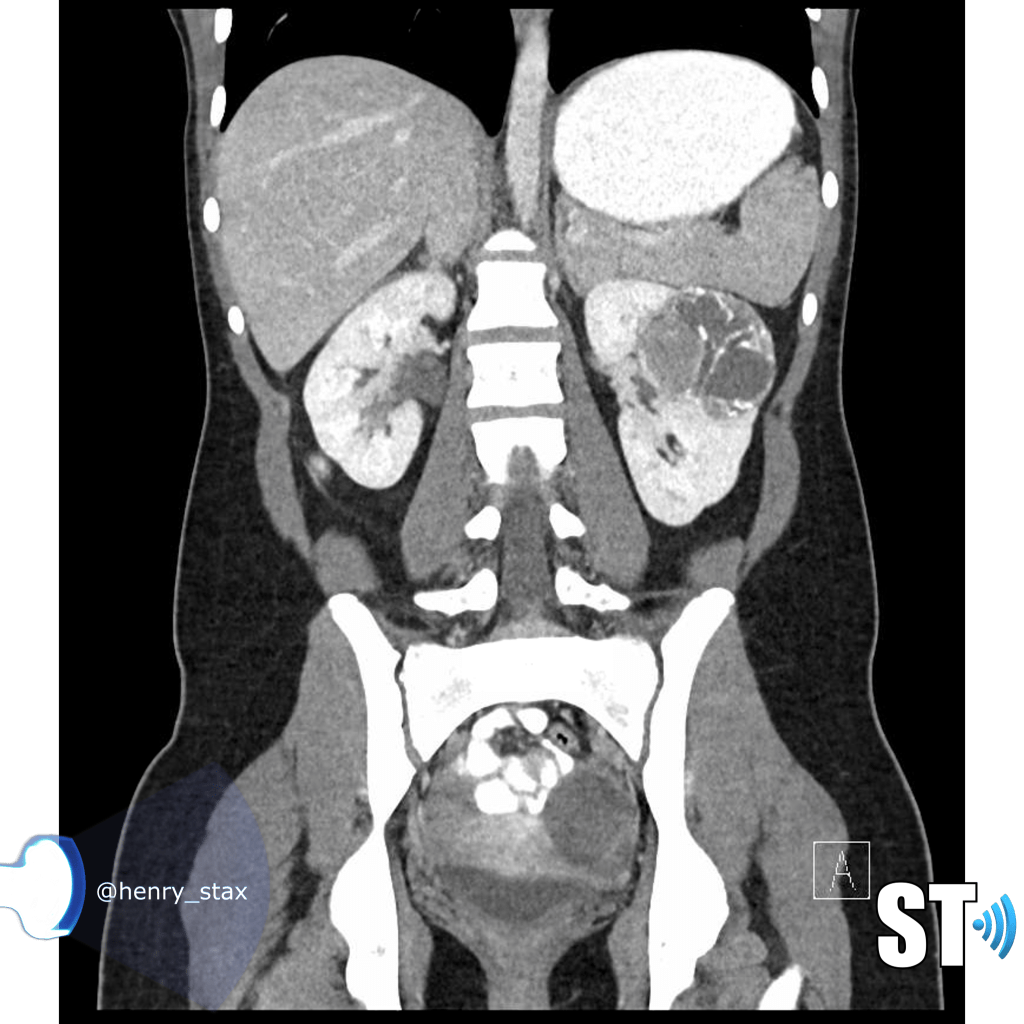
ADPKD
In Autosomal Dominant Polycystic Kidney Disease (ADPKD) the kidneys are normal at birth with cysts developing overtime. By age 30 years, approximately 68% of patients will have visible cysts by ultrasound. Eventually, virtually all patients develop cysts. The disease is transmitted in an autosomal dominant pattern, meaning you only one abnormal gene from one parent.
One abnormal gene from one parent
- Adult
- 4-10% of all cases of ESRF
- Kidneys appear normal early on
- Liver, pancreas and spleen cysts
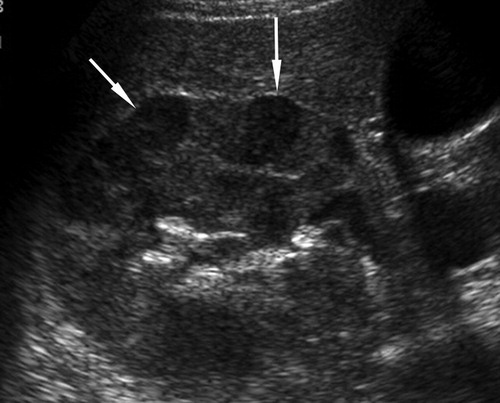
Medullary Sponge Kidney
Medullary sponge kidney is a condition where the collecting tubules in the renal pyramids are ectatic. Withing these tiny cystic spaces calcium salts can accumulate and lead to nephrocalcinosis and/or nephrolithiasis. The Renal pyramids are hyperechoic on ultrasound sometimes with posterior acoustic shadowing.
- benign congenital anomaly
- Cystic dilatation of the medullary pyramids
- Bilateral 70 %
Nephrocalcinosis
- Diffuse medullary calcifications
- Hyperparathyroidism
- Medullary sponge kidney
- renal tubular acidosis
- Hypervitaminosis D
- Sarcoidosis
- hyper/hypothyroidism
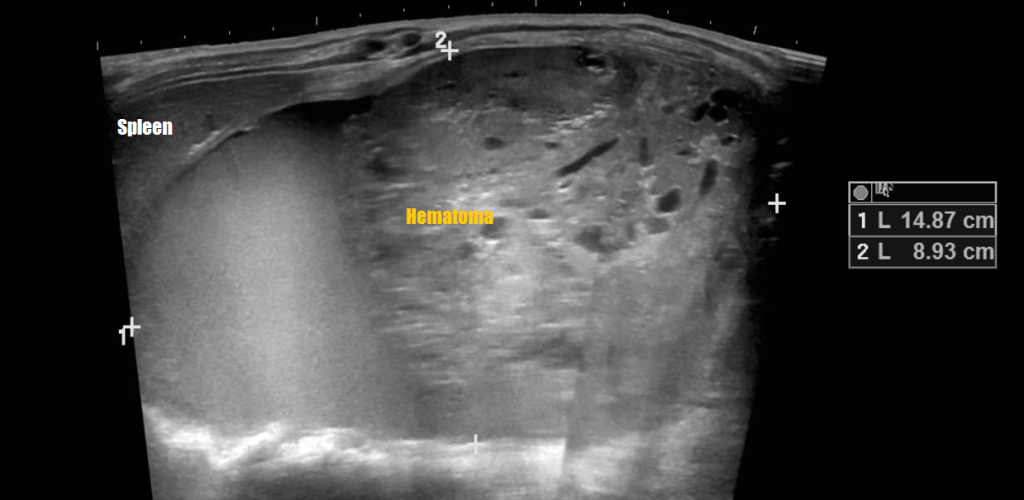
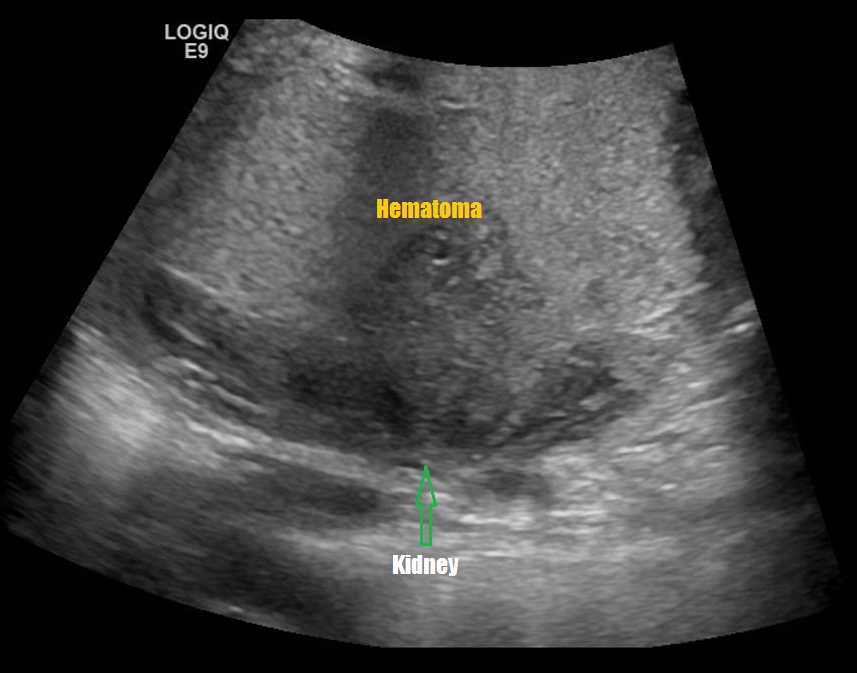
Renal Trauma
Renal trauma accounts for approximately 1-5% of all trauma admissions and as many as 10% of patients who sustain abdominal trauma. Injuries can range from contusions to life threatening injury. The types of trauma include penetrating (gsw, knife), blunt force (mva, sports injury), post procedure etc..
Patients may have abdominal/flank pain on the affected side, hematuria may also be present.
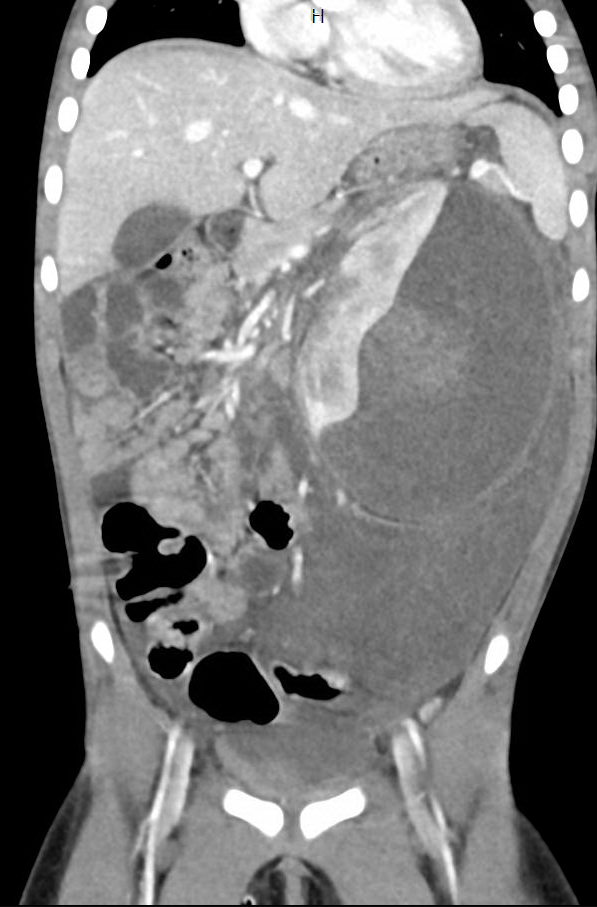
Masses (Malignant and Benign Tumors)
Mesoblastic nephroma (aka renal hamartoma)
- first few months
- Some detected prenatally
- Metastasis rare but has been reported in lungs, brain and bone
- Good prognosis
Wilms Tumor (aka nephroblastoma)
- Most common pediatric renal malignancy
- 87% of renal tumors
- Mean 3 to 4 years
- Bilateral in 4-13% of cases






Multilocular Cystic Nephroma
- Predominantly cystic and septated
- Rare
- Presents typically in the 5th – 6th decades
- Females are predominantly affected

Renal Cell Carcinoma (RCC aka hypernephroma)
- Most common in adults
- If pediatric usually after 11 years old
- solid/cystic, variable echogenicity
- Tumor may invade RV, IVC
Renal Oncocytoma
- Thought to arise from intercalated cells of collecting ducts
- 5-15% of surgical neoplasms
- Central scar, homogenous (non-specific)
Angiomyolipoma
- Benign
- Hyperechoic
- Very common in tuberous sclerosis
- Complications are intratumoral bleeding (hypoechoic areas)

Metanephric adenoma
- Rare, benign
- Range 5 to 83 years (mean 40)
- Can be found incidentally, or with symptoms

Renal Leiomyoma
- Usually found incidentally
- Benign
- Arises from smooth muscle
- Indistinguishable from RCC

Nephroblastomatosis
- Clusters of embryonic metanephric cells
- Give rise to approximately 30-40% of Wilms tumors.
- 2 pathologic subtypes
- perilobar rest (90%)
- intralobar rest (10%).
- Enlarged kidneys, focal masses indistinguishable from Wilm’s
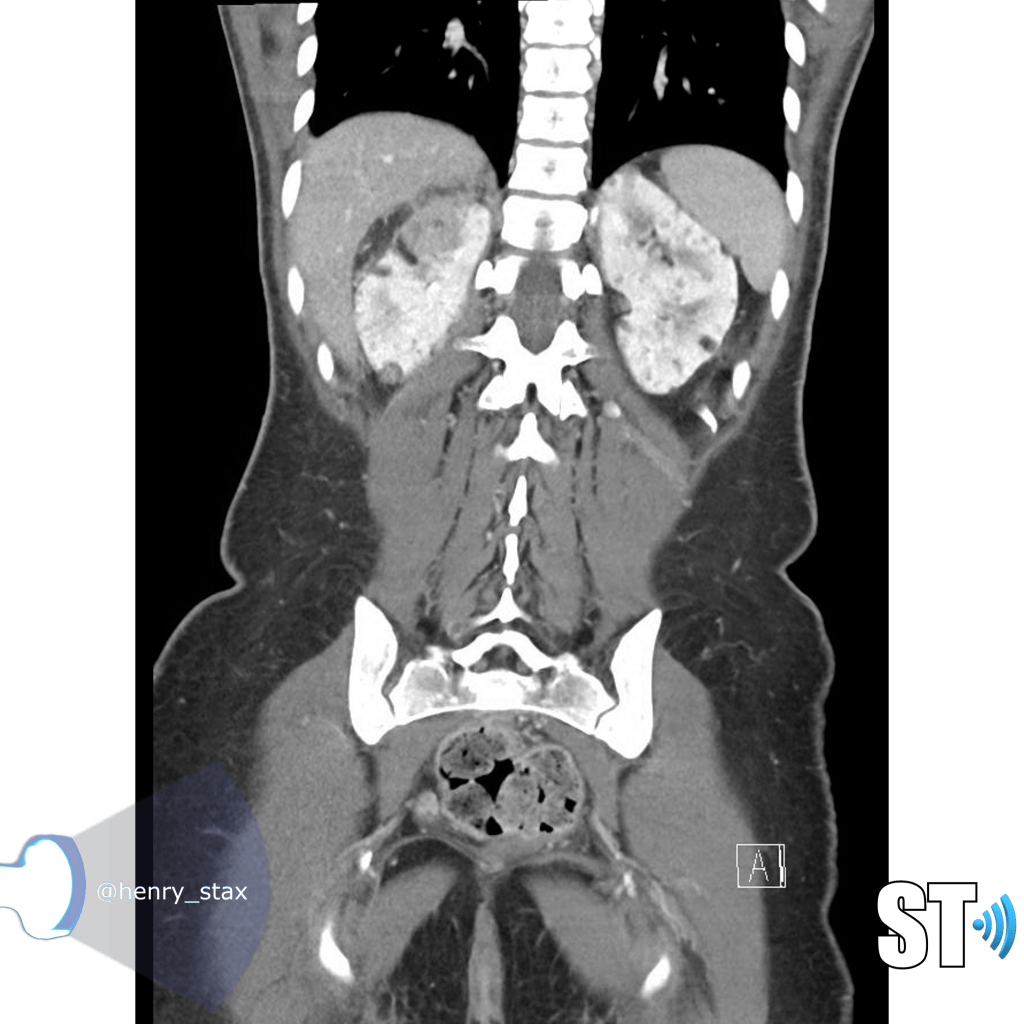
Lymphoma
Renal lymphoma occurs in both primary and secondary forms. The kidney does not have lymphoid tissue, thus primary renal lymphoma is very rare. Most commonly the kidney is affected by hematogenous infiltration. Bilateral involvement is more common. On ultrasound you’ll typically see an enlarged kidney sometimes with ill defined hypoechoic lesions.

Sheila Sheth, Syed Ali, Elliot Fishman
Leukemia
Renal leukemic infiltration is quite common in pediatric patients with leukemia. The infiltration is usually diffuse and bilateral, but can be focal in some cases. As with lymphoma, renal leukemia can be seen on ultrasound as normal kidneys or diffuse nephromegaly.
G Bathla, G Khandelwal, S Singh, V Chowdhury, V Maller
Sources:
Resnick, M. and Rifkin, M. (1991). Ultrasonography of the urinary tract. Baltimore…[etc.]: Williams & Wilkins.
McQuaid, J., Kurtz, M., Logvinenko, T. and Nelson, C. (2017). Bladder debris on renal and bladder ultrasound: A significant predictor of positive urine culture. Journal of Pediatric Urology, 13(4), pp.385.e1-385.e5.
Garfield, Karen. “Simple Renal Cyst.” StatPearls [Internet]., U.S. National Library of Medicine, 4 June 2019, http://www.ncbi.nlm.nih.gov/books/NBK499900/.
Gallant, J., Barnewolt, C., Taylor, G. and Donovan, M. (1997). Radiologic-Pathologic Conference of Children’s Hospital Boston: Bilateral asymptomatic renal enlargement. Pediatric Radiology, 27(7), pp.614-617.
Sheth, S., Ali, S. and Fishman, E. (2006). Imaging of Renal Lymphoma: Patterns of Disease with Pathologic Correlation. RadioGraphics, 26(4), pp.1151-1168.
Bathla, G., Khandelwal, G., Singh, S., Chowdhury, V. and Maller, V. (2009). Renal Involvement In Leukemia: A Report Of Two Cases. The Internet Journal of Hematology, 5(2).

Very interesting and organised notes for a student and are trainee
LikeLike