

Neonatal Neurosonography is a very important and indispensable tool for evaluating pre-term and term neonates for intracranial pathology. It is readily available, portable, relatively inexpensive and safe. Premature infants are at a heightened risk for Intracranial hemorrhage. Up to 67% of pre-term infants born before 32 weeks gestational age develop intracranial bleeds. There is also a variety of intracranial pathologies that can be detected via ultrasound like; hydrocephalus, vascular anomalies, developmental abnormalities, and conditions related to infectious processes.
Anatomy
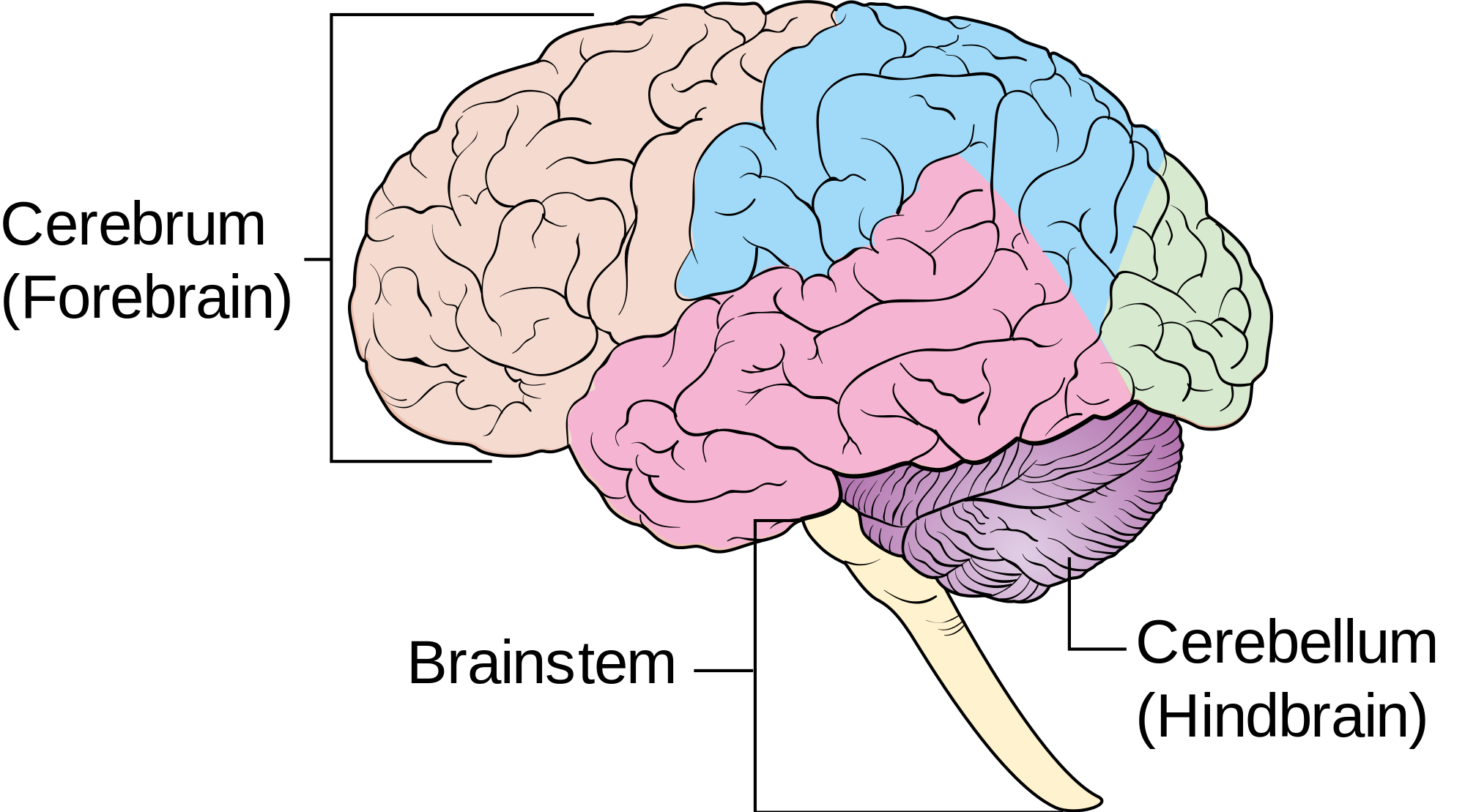
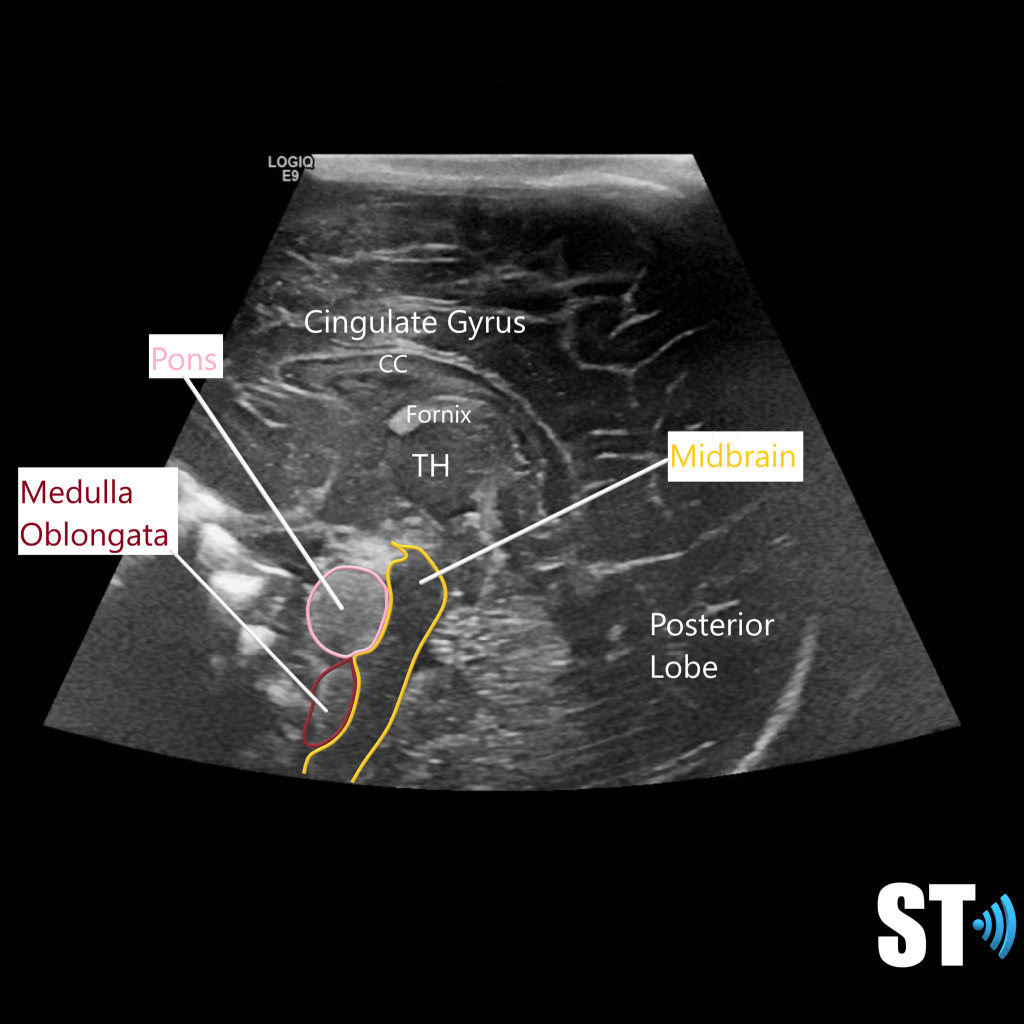
A robust knowledge of neuroanatomy is required for the execution and interpretation of these exams. The brain is divided into 3 main areas the cerebrum, cerebellum and brain stem. It has many convolutions called sulci and gyri that increase the surface area.
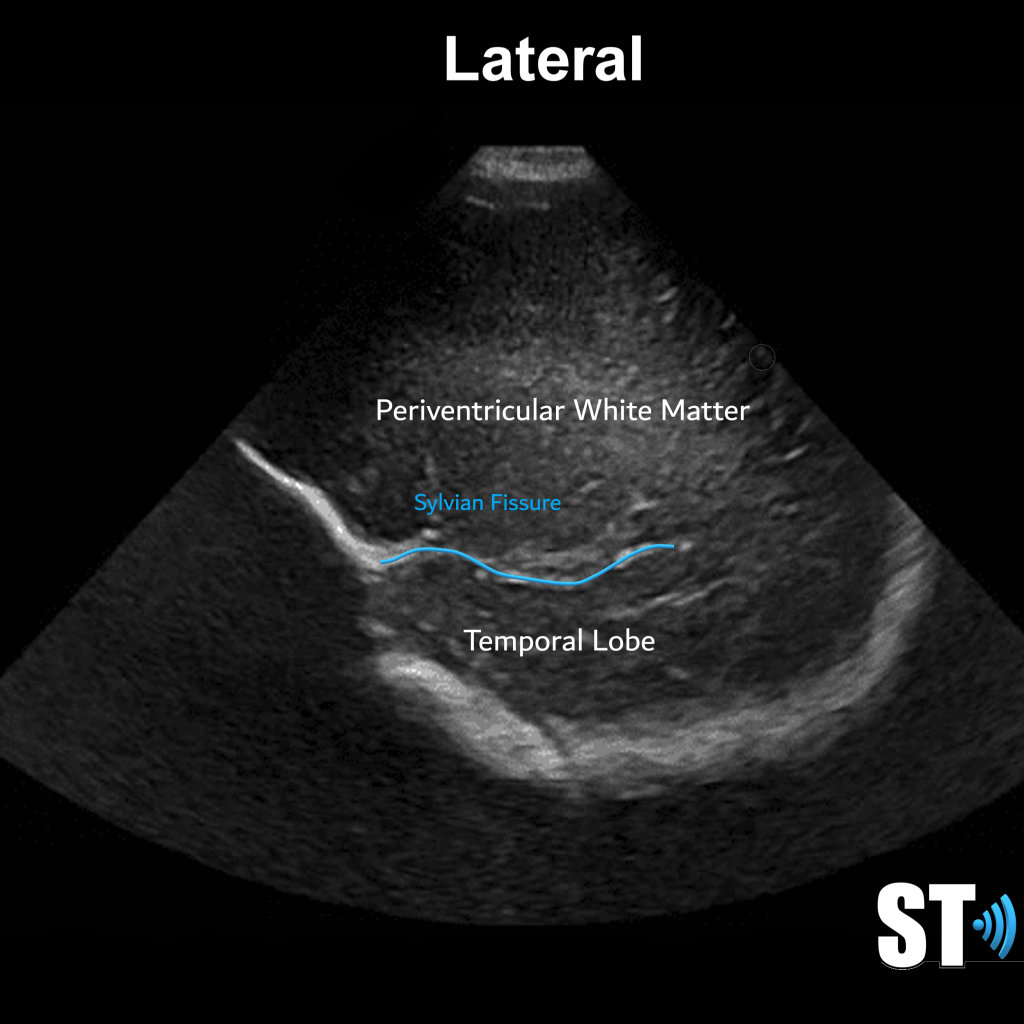
The Cerebrum is the most cephalad portion and consists of 4 lobes: frontal, parietal, temporal and occipital lobes. The separation of these lobes is by way of fissures, which are large grooves. Important ones that pertain to sonographic imaging are the sylvian Fissures, cingulate gyrus and the interhemispheric fissure, which divides the brain into right and left hemispheres.
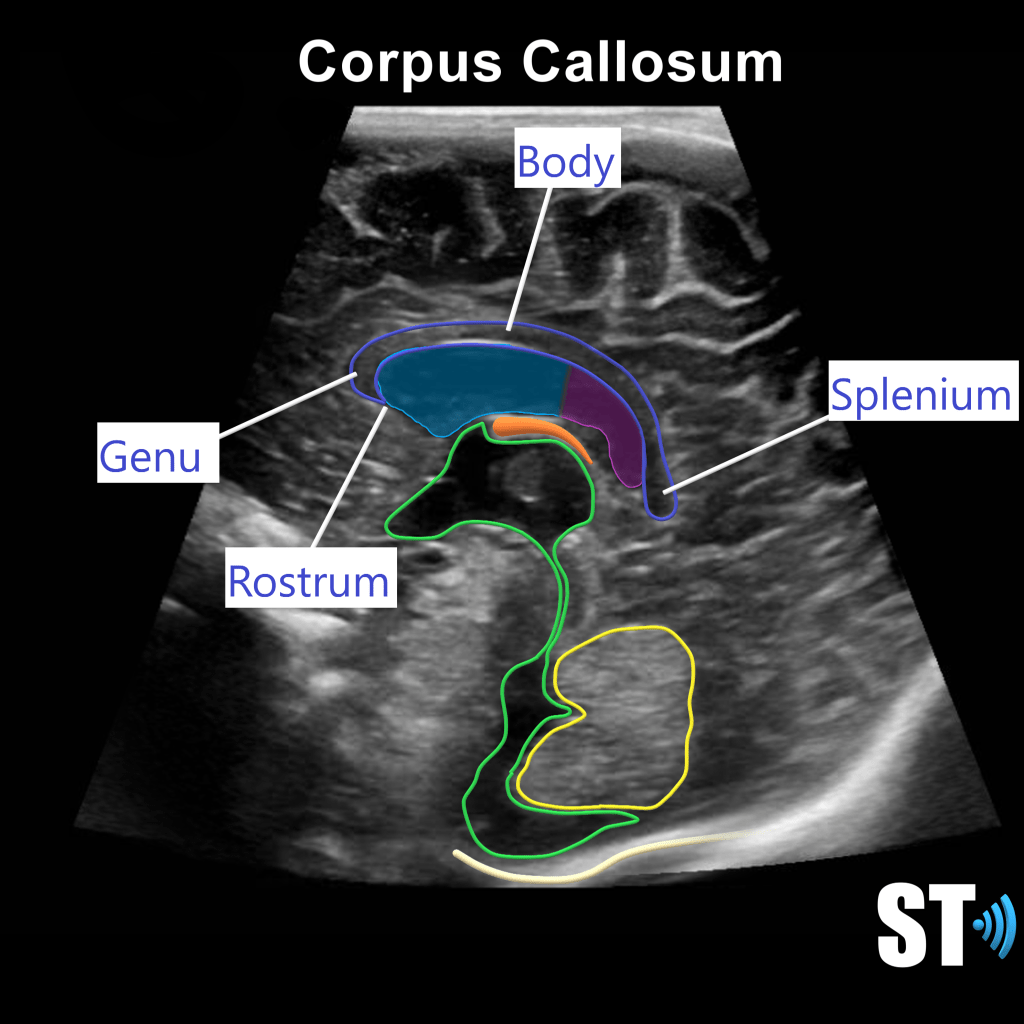
These hemispheres are connected by the corpus callosum (CC), a large bundle of nerve fibers that allow the hemispheres to communicate. There is a fluid filled structure right below that CC called the septum pellucidum. This structure is an important marker in the fetal brain to rule out structural anomalies.
Neonatal Neuroanatomy and Protocol
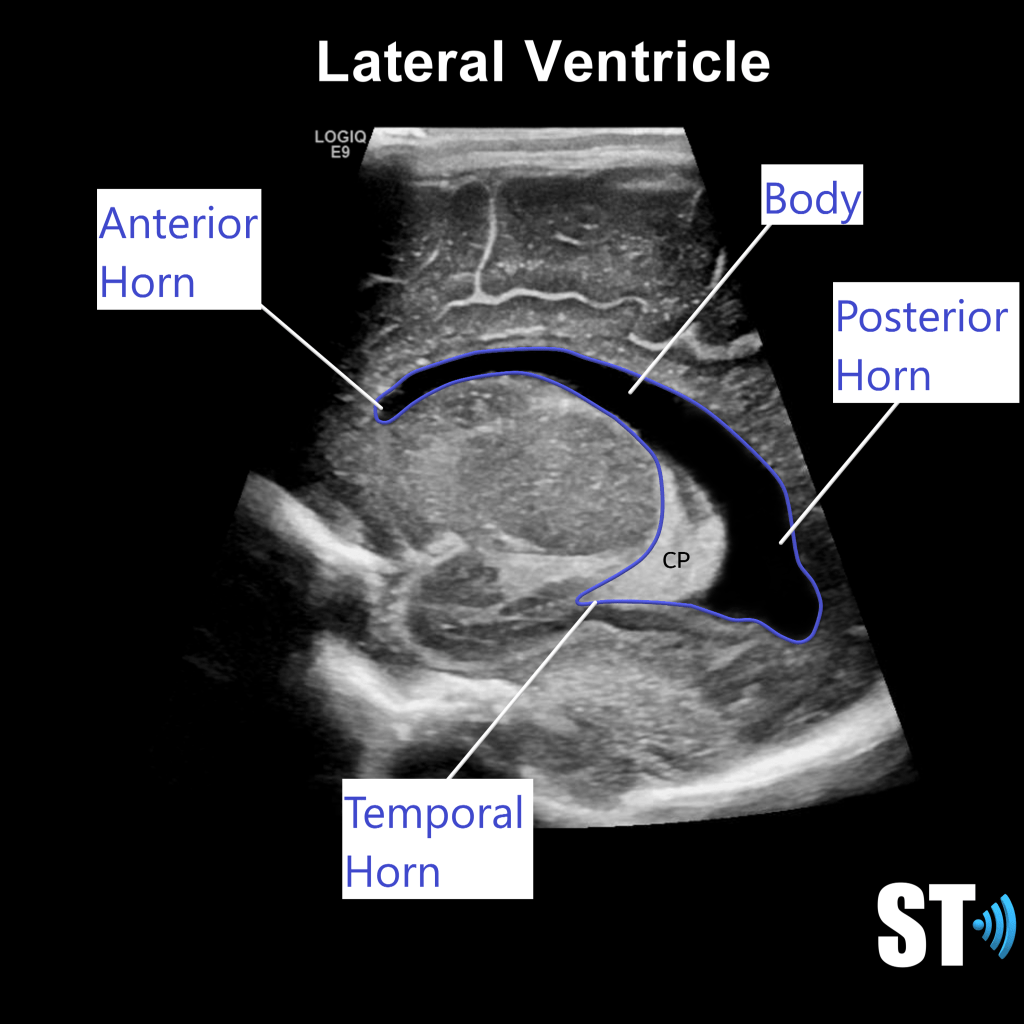
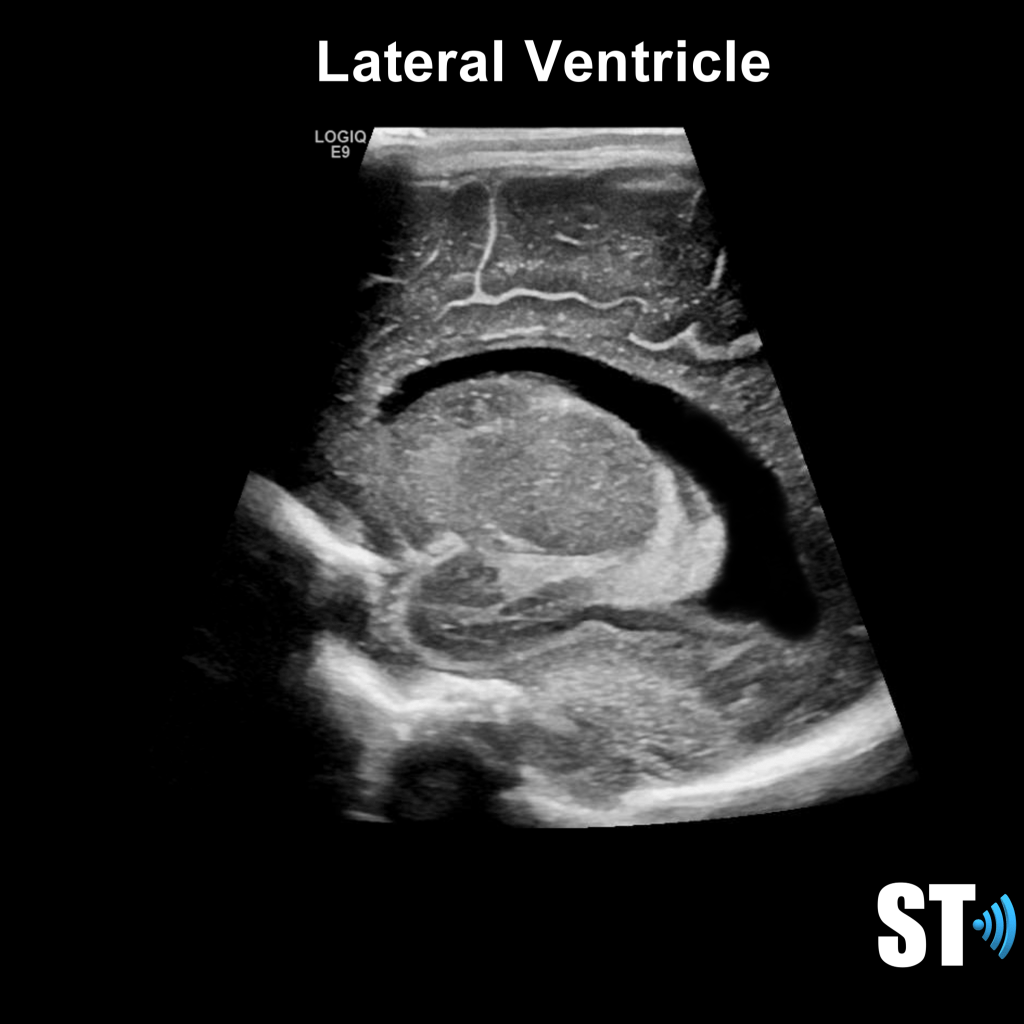
Ventricular System
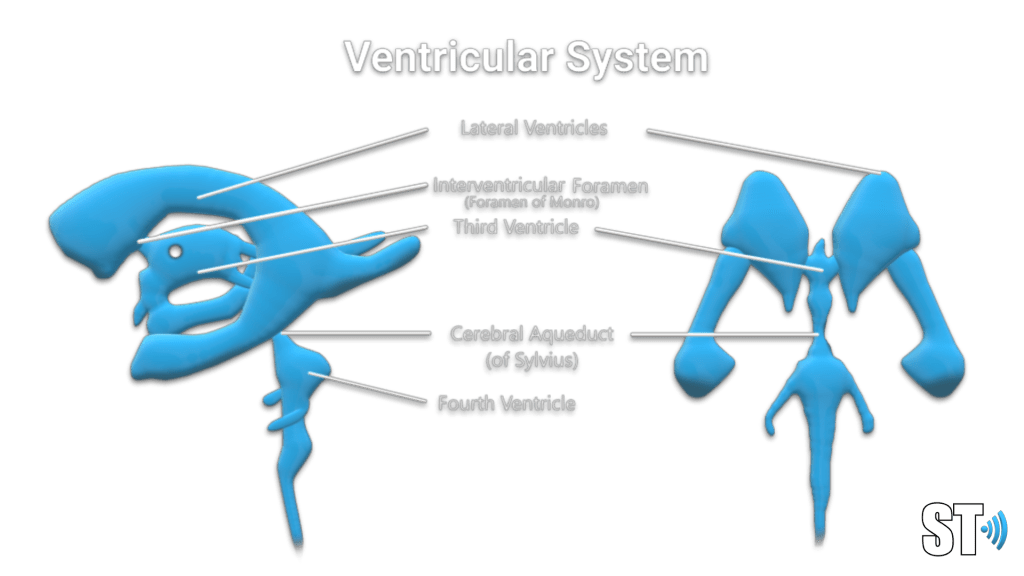
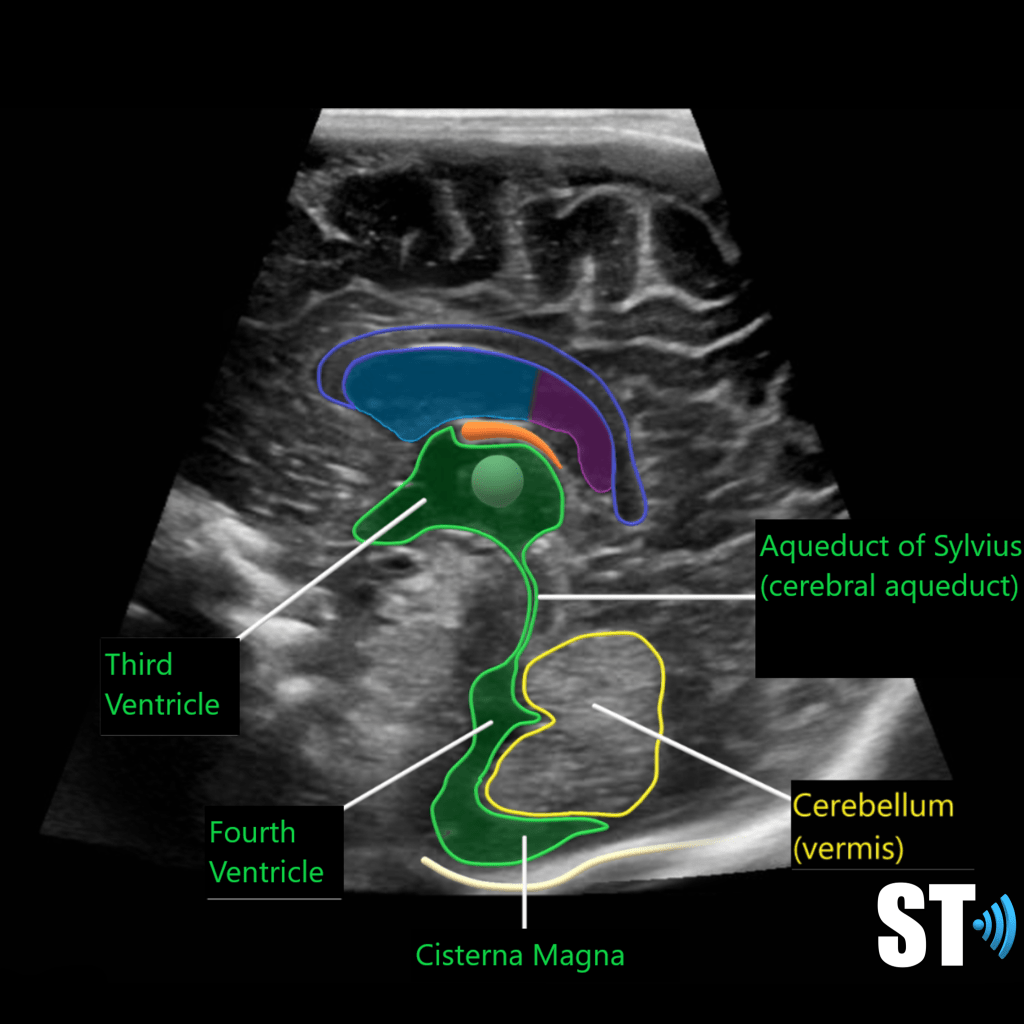
The ventricular system is a series of chamber deep within the brain that collect and allow the flow of cerebrospinal fluid. The main components are the paired lateral, third and fourth ventricles.
Within each ventricle is the choroid plexus which is a network of cells that line the bodies of the lateral ventricles, the roof of the third ventricle and a little bit in the fourth ventricle. The choroid plexus creates the cerebrospinal fluid.
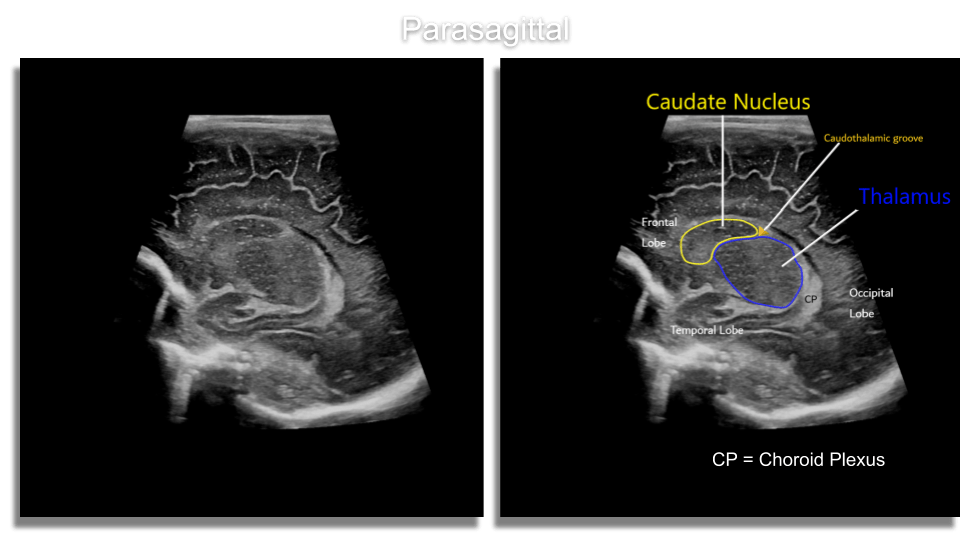
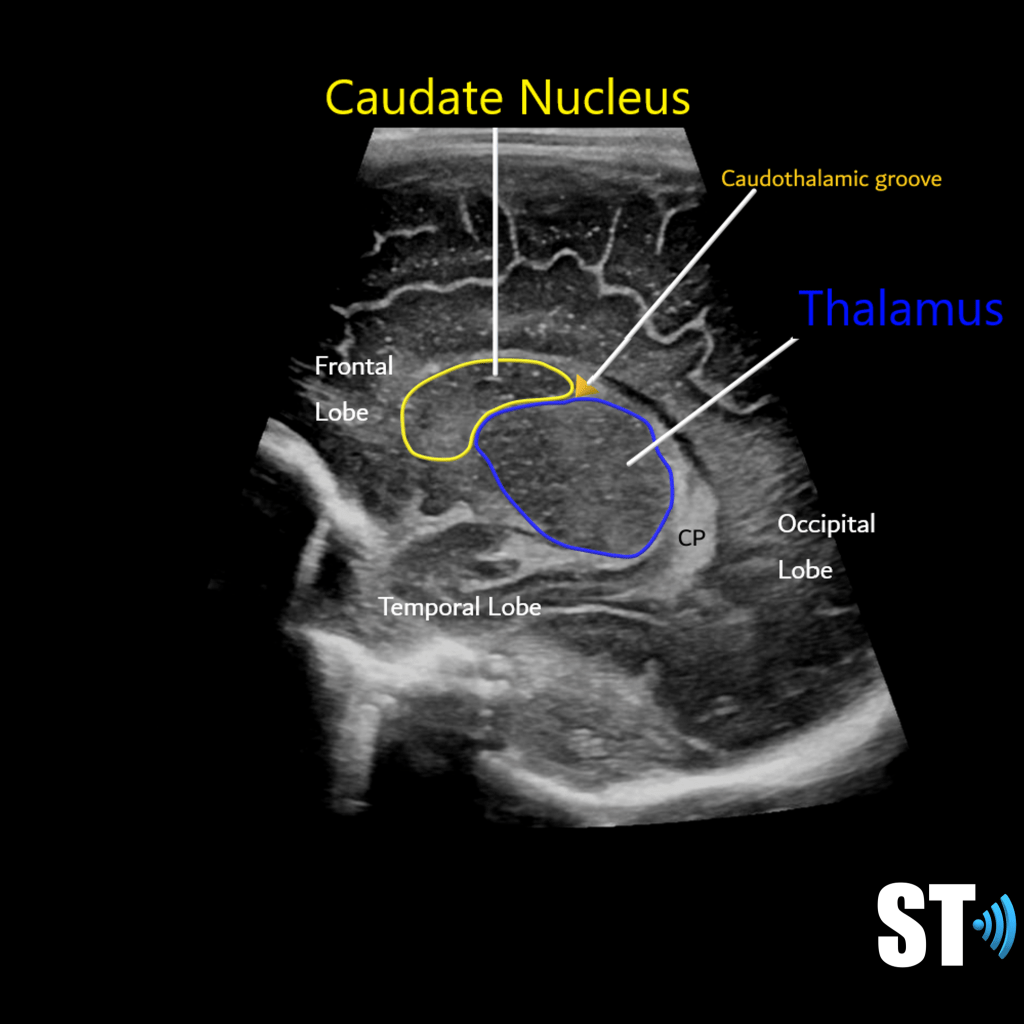
Basal Ganglia
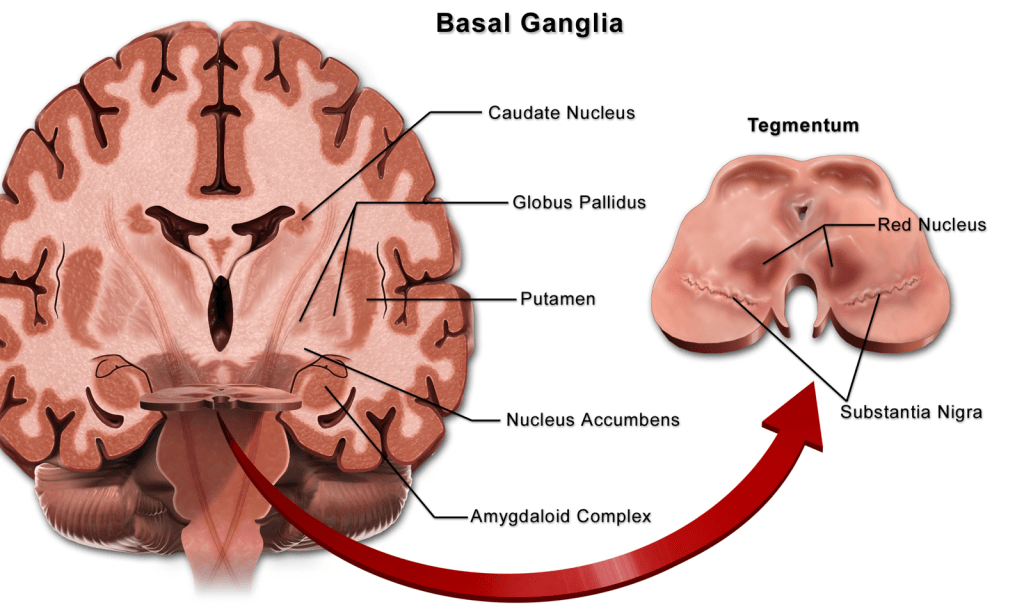
The basal ganglia is a group of grey matter structures found in the base of the brain that relate to the thalamus and are important to movement and coordination.
Sonographically important structures:
Caudate nucleus and thalamus which form the caudo-thalamic groove an area where grade I Hemorrhages occur due to the highly vascularized and fragile germinal matrix which lies just above it in the subependymal (under the ventricular lining), region.
Cerebellum
The cerebellum is another occipital bi-lobe structure which is also important motor control. It is located in the posterior fossa.

Technique
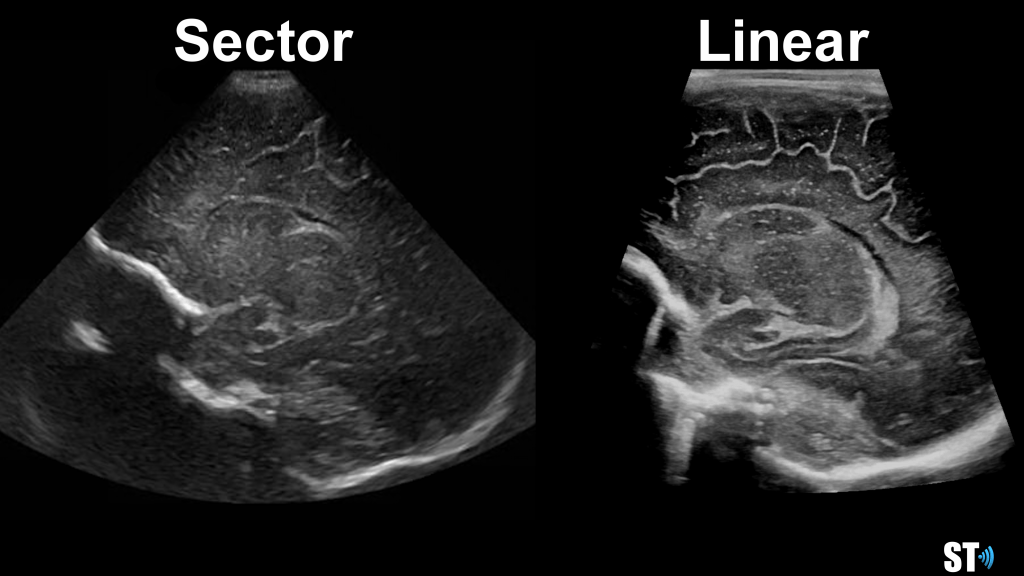
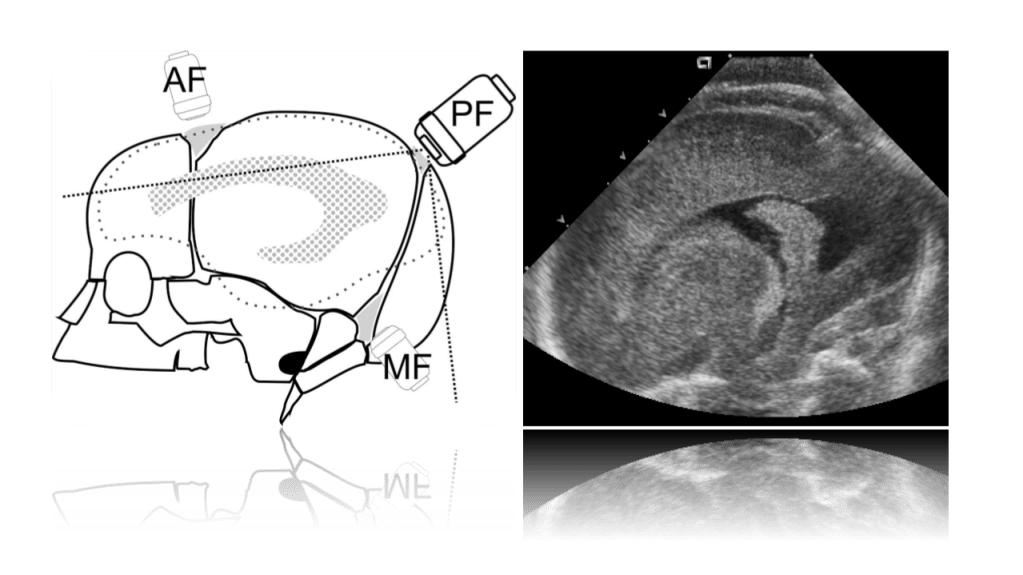
Scanning is usually performed with small footprint high frequency transducers for optimal resolution. The younger the neonate the higher the frequency that can be used. Full term and older babies may require a 5-7 MHz frequency to assure penetration to the deep structures in the brain. Higher frequency linear transducers may be used to evaluate superior cortical structures/lesions and vasculature including the superior sagittal sinus.
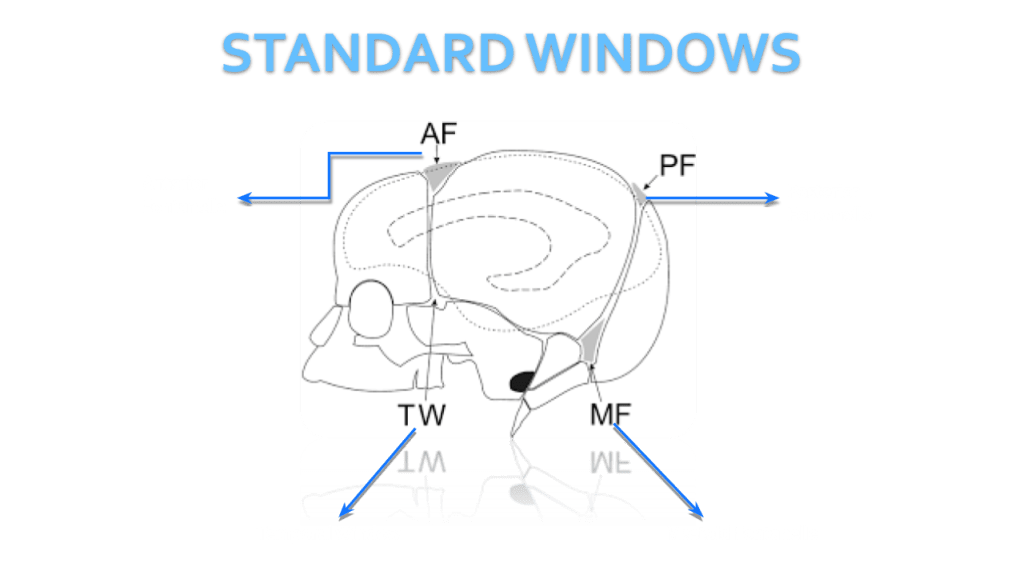
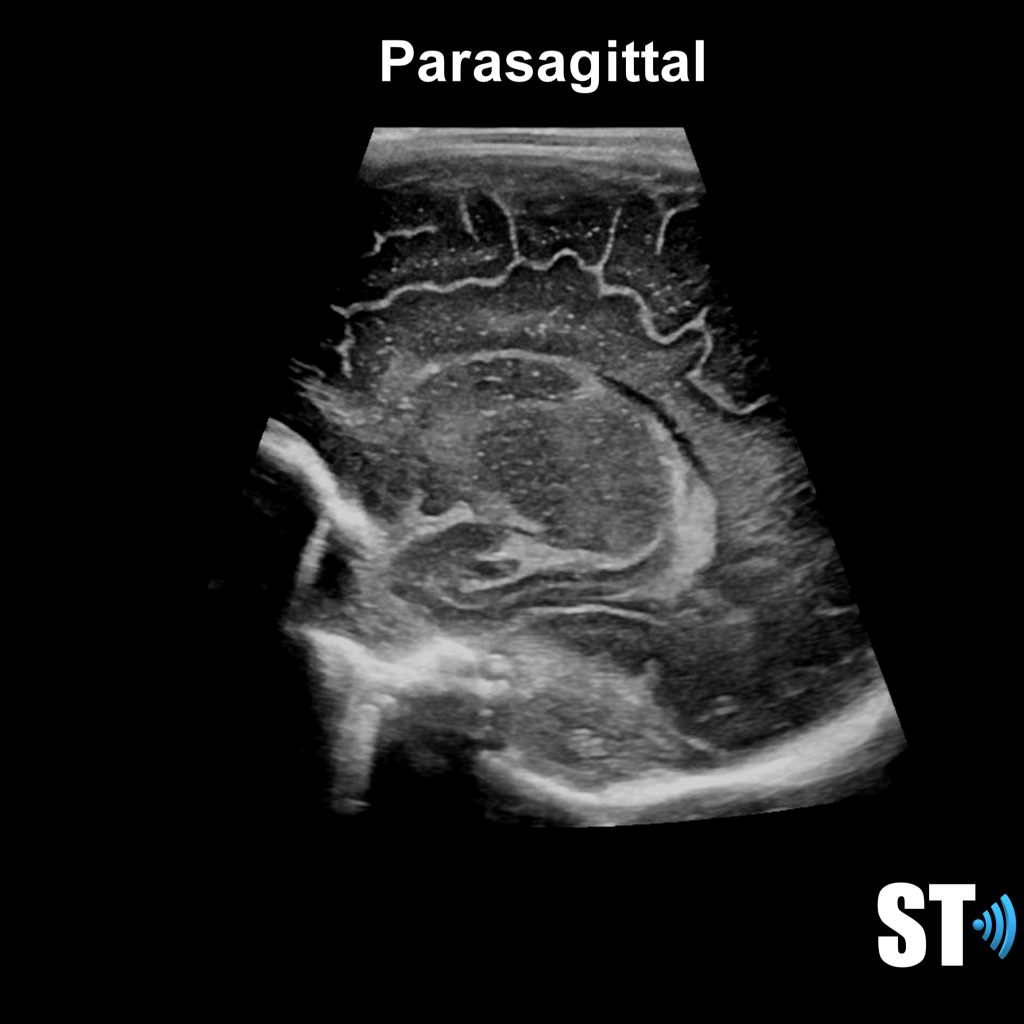
We use primarily the anterior fontanelle using a coronal, sagittal and parasagittal views. Also we scan through the mastoid fontanelle (for the posterior fossa and cerebellar views) and posterior fontanelle (for posterior structures especially the occipital horn to detect dependent hemorrhage) and temporal views for further evaluation.
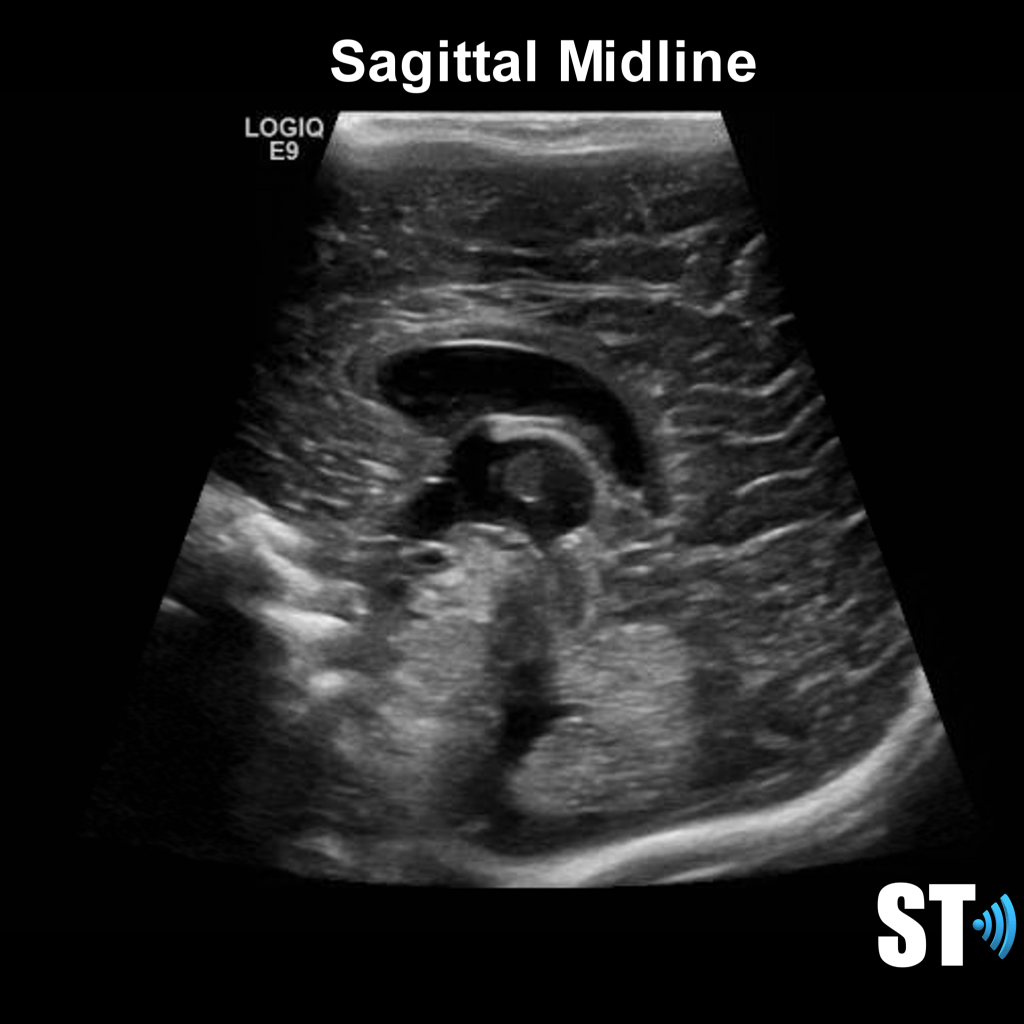
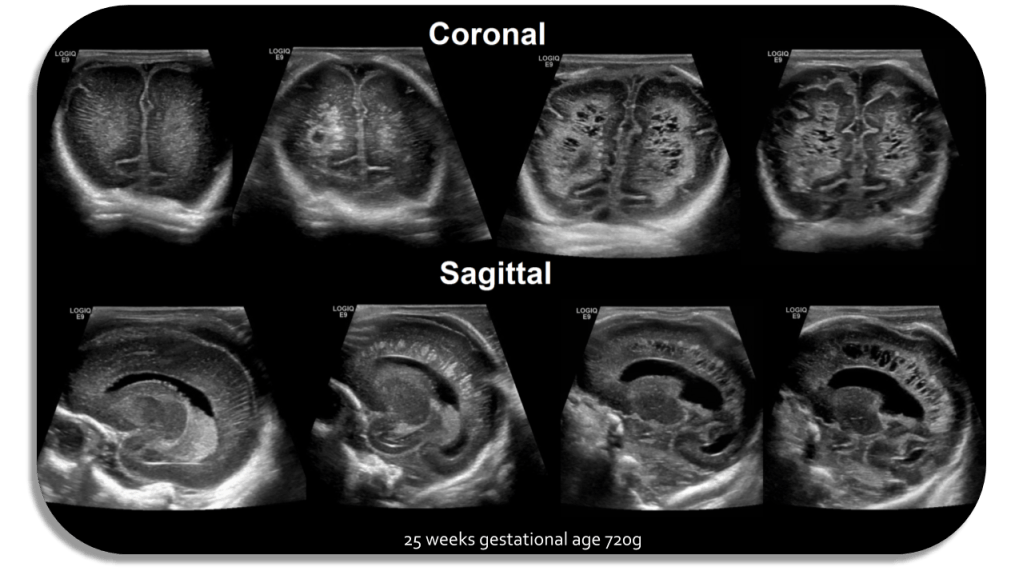
Sagittal Anterior Fontanelle Views



Coronal Anterior Fontanelle Views
The exam should be done with the patient in the supine position, though you may encounter patients in various positions depending on their care. If the patient is in lateral decubitus the exam can still be done.
Patients may have multiple lines including venous and arterial lines, nasogastric and endotracheal tubes. Extra care must be taken when scanning these babies to avoid potentially dislodging of these catheters.
Posterior Fontanelle
Periventricular white matter should be less echogenic than the choroid plexus. The infant brain that is <32 weeks gestational age will have a smoother appearance with less sulci and gyri. 36 weeks and greater more sulci and gyri and the ventricles are more slit like.
Intracranial Hemorrhage of Prematurity
Intraventricular hemorrhages aka Germinal Matrix/Subependymal bleeds are believed to happen due to poor autoregulation of premature infants, sudden changes in pressure or oxygen saturation can cause sudden reperfusion which ruptures of the tiny delicate vessels within the germinal matrix.
Etiologic Factors
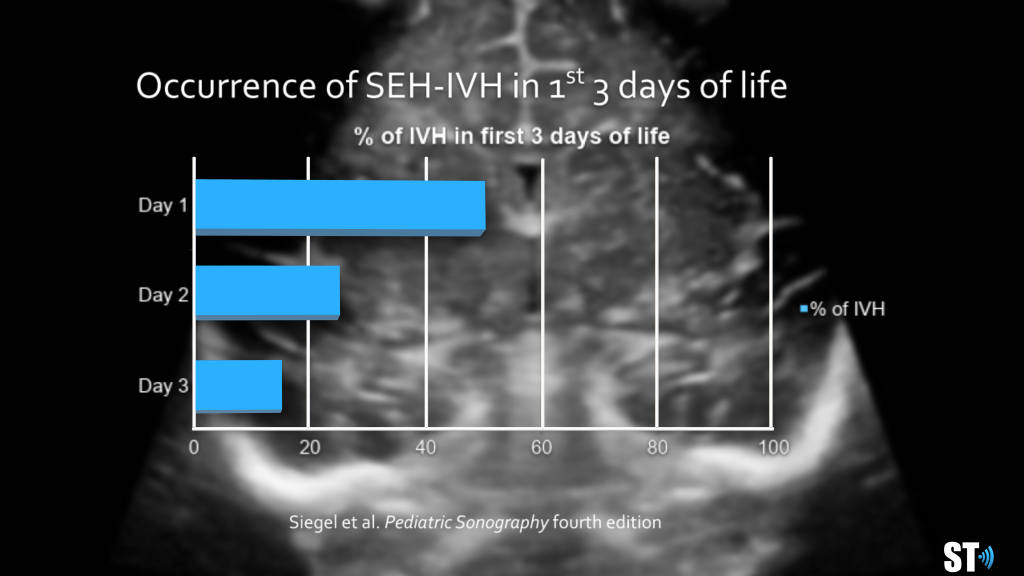
Most of the Bleeds occur early
Day 1 50%
Day 2 25%
Day 3 15%
Day 4 10%
95% of all bleeds occur by day 9
The intraventricular hemorrhage is typically categorized into 4 grades:


A subependymal (grade I) bleed will eventually liquify and undergo cystic degeneration. 80% extend into the Intraventricular region (grade II). 15% of bleeds will also develop in the intraparenchymal hemorrhages (grade IV). It was thought that intraprenchymal bleeds started in the germinal matrix as grade I’s and progress, but now it is believed that they occur from venous infarcts.

Sequlae of ICH
Hydrocephalus
Cysts (porencephalic cysts and periventicular leukomalacia)
Encephalomalacia (necrosis of white matter with liquefaction and cavitation) ventricular dilatation.
- 70% infants with IVH resolve or be mild
- 15% will be severe
- 15% or less require shunts
Hypoxic-ischemic encephalopathy is one of the most common causes of cerebral palsy and other severe neurological deficits in children, occurring in 2-9 of every 1000 live births.
Hypoxic Ischemic Encephalopathy
Perinatal asphyxia results in the loss of normal cerebral autoregulation and diffuse brain injury.
- Major cause of morbidity and mortality in neonates
- Estimated prevalence of 2-4 per 1,000 live births
- Redistribution of blood to the brain may lead to multi-organ failure
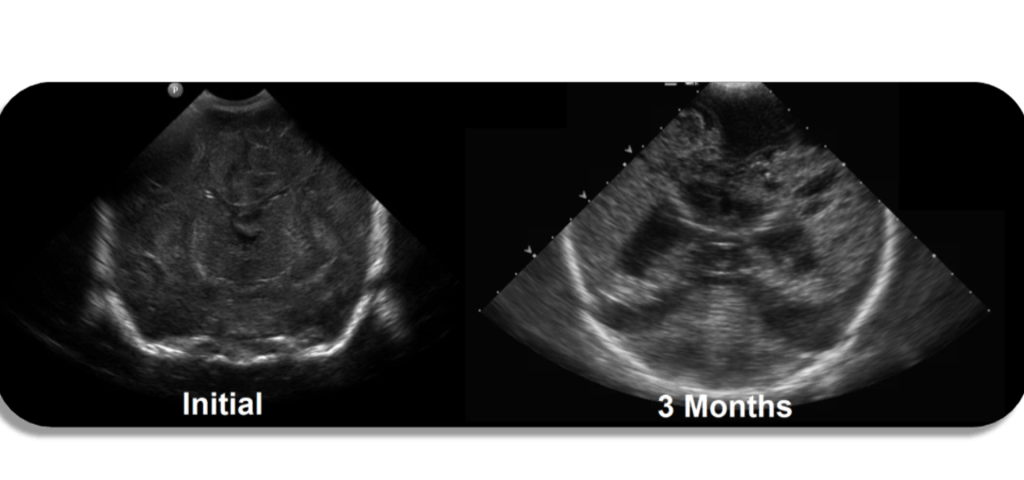
- Initial sonogram typically normal
- Follow US can show echogenic lesions which progress to cystic degeneration (encephalomalacia)
Sonographically you can see echogenic brain parenchyma with loss of differentiation of the grey and white matte, findings which are suggestive of edema. In the acute phase after a hypoxic ischemic event the brain will appear normal on ultrasound.
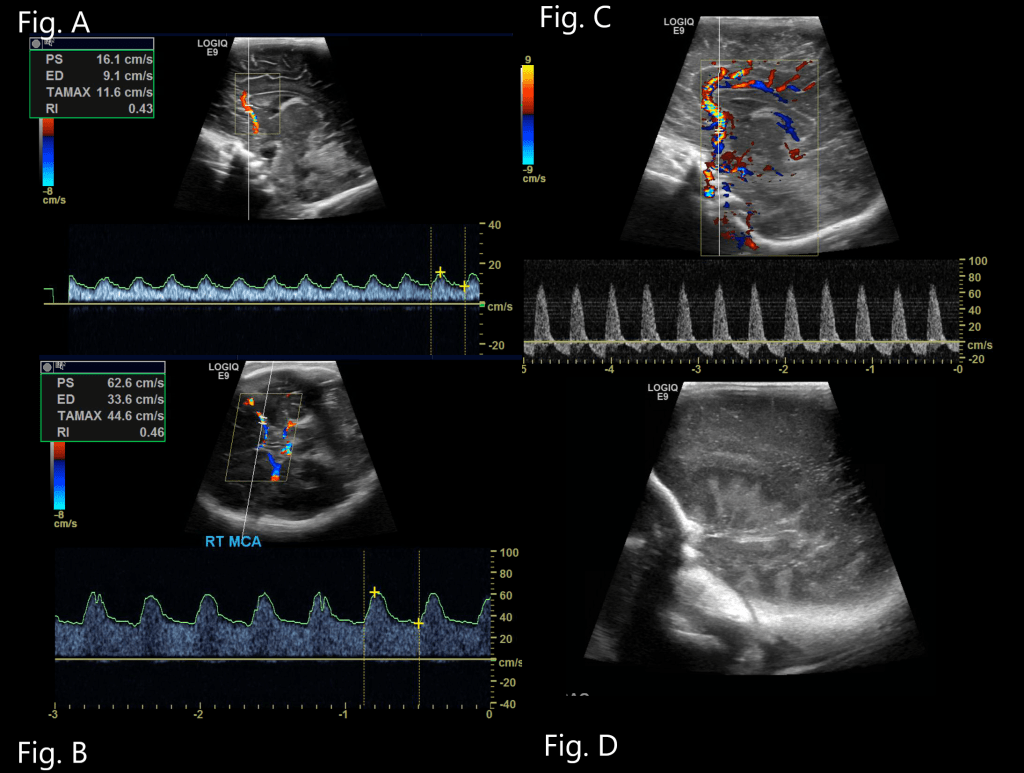
Resistive Index
Resistive index of the middle cerebral arteries, Loss of cerebral autoregulation in HIE can predispose to reduced/absent diastolic blood flow in cerebral arteries leading to increased RI (>0.80) or elevated diastolic flow due to arterial vasodilation resulting in reduced RI. Decreased RI has been well documented in asphyxia and found to increase the risk of death or cerebral palsy by 23.4 times.
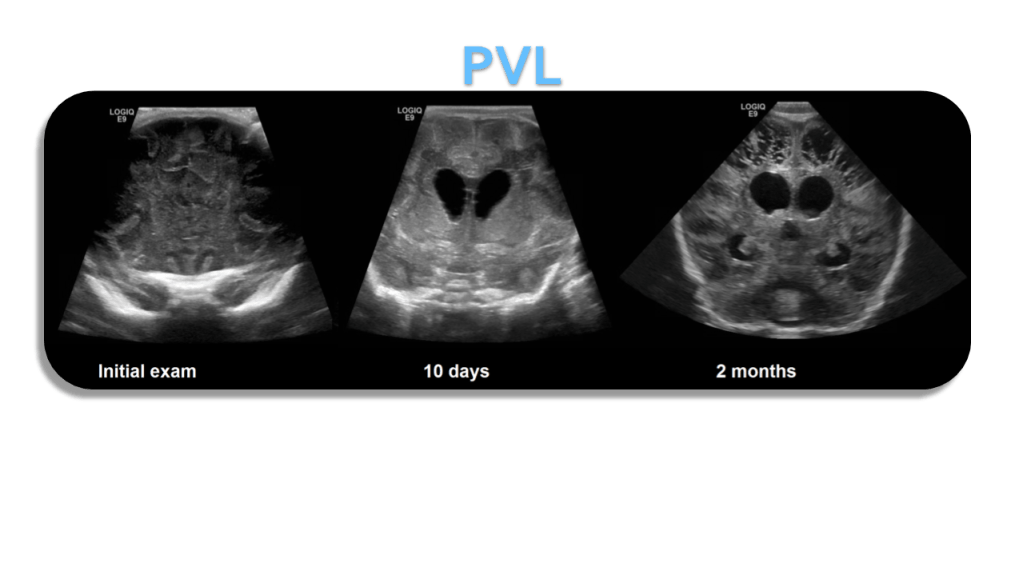
Periventricular Leukomalacia (PVL)
- Periventricular white matter normally hyperechoic but < choroid plexus
- Increased echogenicity around the ventricle (white matter ischemia)
- Progresses to cystic spaces that replace normal brain
- (white matter necrosis)
- Cystic changes typically appear 2-6 weeks after vascular insult
- Significant neuro-motor impairment follows
Periventricular leukomalacia (PVL), or white matter injury of prematurity affecting the periventricular zones, typically results in cavitation and periventricular cyst formation.
PVL is most common in premature neonates (less than 34 weeks gestational age with a median gestational age of 30 weeks) and <1500 grams at birth.
Cerebral palsy and intellectual disabilities are common sequela of PVL.
It is thought to occur as a result of hypoxic-ischemic lesions resulting from impaired perfusion at the watershed areas, which in premature infants are located in a periventricular location.
Early on the periventricular white matter may increase in echogenicity ultimately resulting in cyst formation.
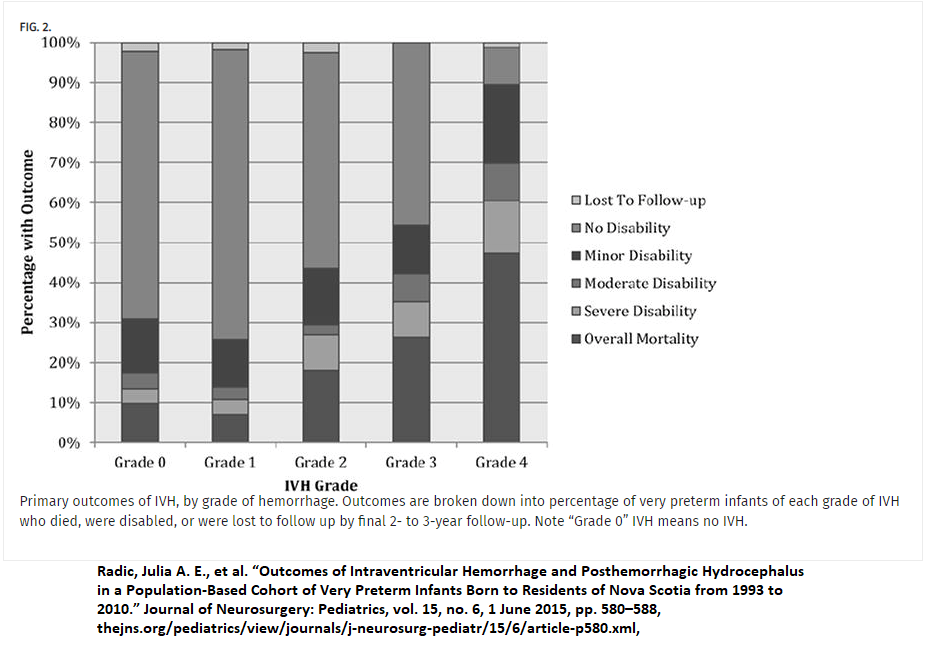
Outcomes of Bleeds by Grade
Sources:
“State-of-the-Art Cranial Sonography: Part 1, Modern Techniques and Image Interpretation : American Journal of Roentgenology: Vol. 196, No. 5 (AJR).” State-of-the-Art Cranial Sonography: Part 1, Modern Techniques and Image Interpretation : American Journal of Roentgenology: Vol. 196, No. 5 (AJR). N.p., n.d. Web. 07 Nov. 2016.
Ultrasound Q. 2002 Jun;18(2):89-114.
Intracranial neonatal neurosonography: an update.
Benson JE1, Bishop MR, Cohen HL.
Radic, Julia A. E., et al. “Outcomes of Intraventricular Hemorrhage and Posthemorrhagic Hydrocephalus in a Population-Based Cohort of Very Preterm Infants Born to Residents of Nova Scotia from 1993 to 2010.” Journal of Neurosurgery: Pediatrics, vol. 15, no. 6, 1 June 2015, pp. 580–588

Excellent images and explanation. Kindly mention normal PSV, RI values in ACA, MCA in preterm and term neonates and their significance. Awaited for your expert opinion. Thank you.
LikeLike
Thank-you for your excellent teaching.If I could request you to teach on location of MCA and ACA and how to locate them during doppler
LikeLike
wonderful images and explanations, looking forward to learning more from your teaching and skills
LikeLike
Fantastic teaching and visuals as always
LikeLike