

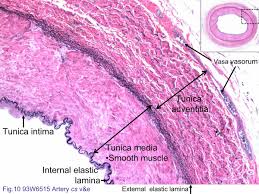
Abdominal Aortic Aneurysm is a focal dilatation of the Aorta caused by degeneration of the tunica media (middle connective layer of the arterial wall).
It is a relatively common condition. It is most commonly seen in white males over 50 years of age. The normal size of the Abdominal Aorta is 1.5 cm. AAAs larger than 5.0-5.5 cm should be electively repaired.


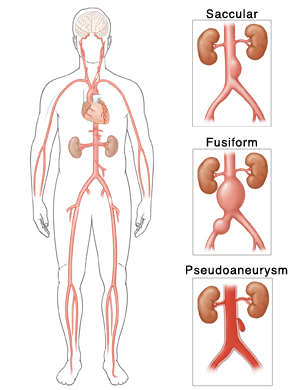
Types
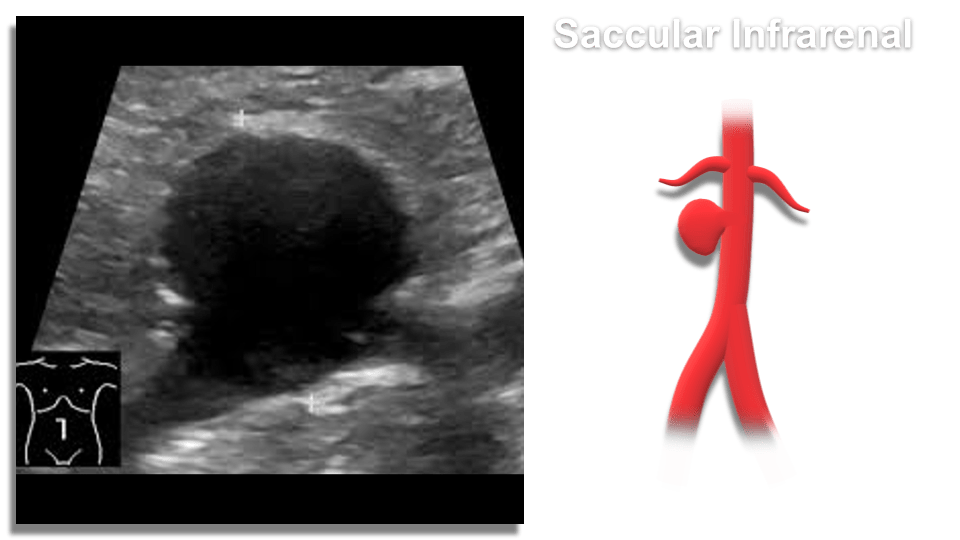
- Saccular – spherical in shape, appear like a pouch or sac from the vessel and are often filled with thrombus within the arterial wall (intramural)
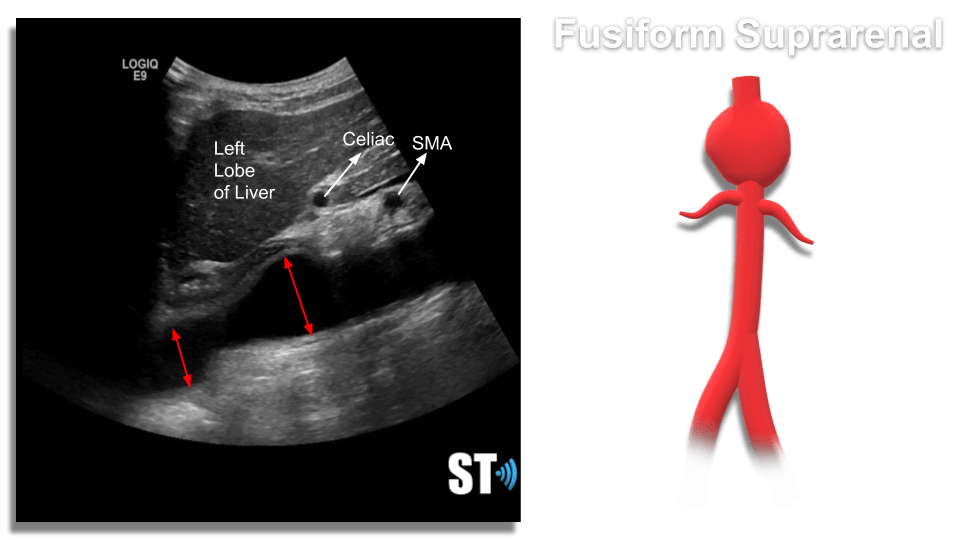
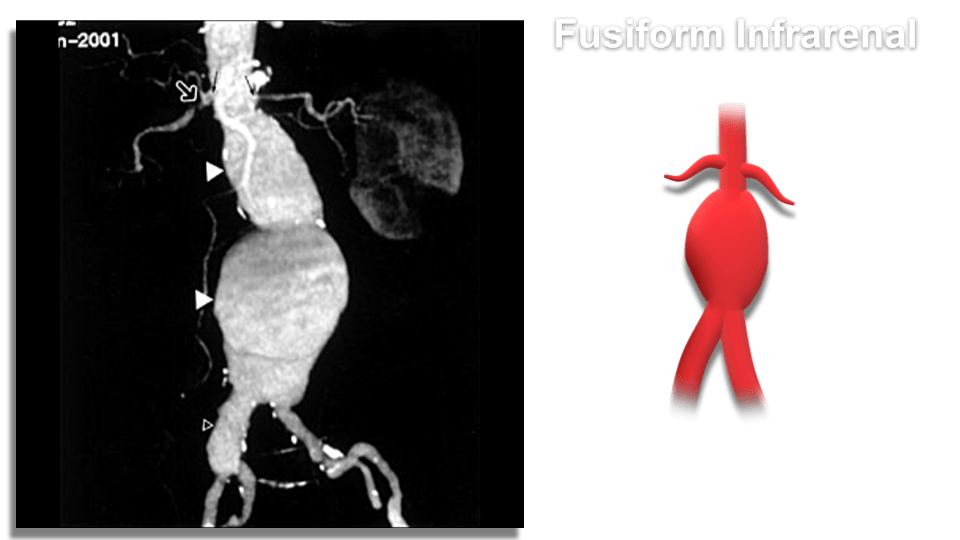
- Fusiform – Dilatation that spans a larger length of the vessel
Pseudoaneurysm – Typically the result of direct trauma or international procedure where the arterial wall is punctured leading to a focal ballooning out connected to the main vessel by a stalk, or neck. Not common in the abdominal aorta, typically seen in femoral arteries after cardiovascular procedures.
Symptoms
Abdominal aortic aneurysms are typically asymptomatic. On occasion there will be a palpable, pulsatile mass in the abdomen. In symptomatic aneurysms the risk of rupture is high. Rupture is a surgical emergency usually with catastrophic consequences, hypovolemia and death soon follow rupture with a mortality rate up to 90%.
Scanning
Patients should fast overnight to eliminate excess bowel gas. Scan the patient supine and lateral decubitus. Scan the Aorta in sagittal and transverse including grayscale, color doppler and spectral waveform analysis. Document proximal, mid and distal aorta and bilateral Iliac arteries including anteroposterior measurements.
Henry Suarez RDMS, RVT
Risk factors include;
- hypertension
- smoking
- atherosclerosis
- males 65 years or older
- Marfan’s syndrome
Aneurysms >3 cm in size gradually enlarge at rate of 0.2 -0.8 mm/year. There is a high risk of rupture once the aneurysm reaches 5 cm. A 7-cm AAA has a 19-32% rate of rupture per year.
