

Renal artery doppler is a powerful tool for the diagnosis of Renal Artery Stenosis (RAS). One of the more involved exams in the sonographers arsenal, learning the proper anatomy and techniques can make the process a challenging yet pleasurable one.
Indications
- Hypertension
- Abdominal bruit
- Known renal artery stenosis follow up
- Elevated BUN and creatinine
- Hematuria (Nutcracker Syndrome)
Anatomy
Aorta
The Aorta is the largest artery in the human body, it begins at heart and branches out to supply oxygenated blood to all the viscera and extremities. It’s main abdominal branches are the Celiac Trunk, Superior Mesenteric Artery, bilateral Renal Arteries and Inferior Mesenteric Artery.
 A.
A. B.
B. C.
C. D.
D. E.
E.- A. Diagram of Aorta, B. Coronal gray-scale image of Aorta and Renal Arteries, C. Proximal sagittal Aorta, D.Mid to distal coronal Aorta with bifurcation, E. Proximal sagittal Aorta with color doppler
Renal Arteries
The renal arteries are paired blood vessels that arise from the mid aorta. The right renal artery is typically longer than the left due to the anatomical location of the aorta being more lateral to left of the body. It courses behind the IVC, which can be used as a window in difficult patients.

.

There is usually one on either side, though multiple renal arteries are quite common and occur in 14-25% of the population (though some studies state more). There can be duplicate, three or more. Main Renal arteries usually enter the kidney at the hilum, though accessory vessels may enter at the poles or other surface of the renal parenchyma.
Renal arteries have low resistance waveforms. 20 % of the cardiac output is in the renal system at any given time.

Intrarenal Arterial Anatomy consists of an arbor like network of vessels coursing throughout the kidney. Once the renal artery enters the kidney it divides into Segmental arteries (usually 5), then further divides into Interlobar, Arcuate and finally Interlobular at the outer reaches of the cortex.



Inferior Vena Cava
The inferior vena cava is the largest abdominal vein receiving deoxygenated blood from the Kidneys, Liver, Spleen and Gastrointestinal system among others.
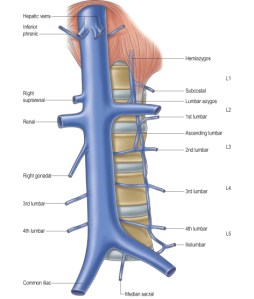



Renal Veins
The renal veins are paired blood vessels that return blood back to the IVC. The left renal vein is the longer one and courses between the superior mesenteric artery and aorta. It is important to visualize these vessels to rule out Renal Vein Thrombosis, or Nutcracker syndrome.


Technique
- Patient NPO 8-12 hrs.
- Transducer 5 mHz curved linear for small patients/pediatrics
- Explain the importance of breath holding (very important)
- Pillow under side
- Small sample volume center stream
- Color, Power Doppler
- Increase sweep speed



AIUM Renal Doppler protocol
Approach
Anterior
With the patient in a supine position you can approach the renal vessels just below the epigastrium. In an axial plane you will view the renal arteries in a longitudinal orientation. In this approach you will have to angle your probe or tilt it in order to get good angles of insonation. If you cross over and use the liver as a window you can achieve a good approach for color and pulsed wave doppler. When using an angle make sure to not pass 60 degrees, preferably staying within the 45 degree. You will want to capture gray-scale, color and pulsed wave doppler imaging, while taking waveform analyses at the proximal, mid and distal renal artery.
As stated before the RRA will be located posterior to the IVC. The LRV will be sandwiched between the Aorta and SMA.
Flank
With the patient in lateral decubitus you will be able to achieve the flank or coronal approach and view both renal arteries and veins completely from vessel to hilum. A rolled towel may be placed under the side opposite to your scanning and the ipsilateral arm raised to further “open” the ribs to allow for better windows. It is also a great approach for accurate doppler signals, being at zero degrees to the sound beam. One view that is achievable is the “banana peel sign” which shows the aorta and bilateral renal arteries and gives the appearance of a peeled banana.
Parameters
- Peak Systolic Velocity (PSV)
- End Diastolic Velocity (EDV)
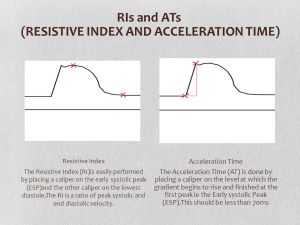
- Resistive Index (RI) *PSV-EDV/PSV* <0.70
- Acceleration Time (AT)
- Renal Aortic Ratio (RAR) *PSV Renal Artery/PSV Aorta* < 3.5
- Aliasing (Qualitative)
Renal Artery Stenosis
RAS causes renovascular hypertention, 5% of patients with hypertension are due to RAS. It is typically the result of atherosclerotic plaque (up to 75%). RAS lesions/plaques are usually found in the ositium (renal artery origin 95% of the time). PSV’s higher than 180 cm/s are diagnostic of stenosis, whereas velocities 200 cm/s and higher are predictive of 60% stenosis. You will also see aliasing (color mosaic), post stenotic turbulence and tardus parvus waveforms at the hilum and in the parenchymal vessels.
Direct Criteria for RAS
- PSV > 180 cm/s (200cm/s 60% stenosis)
- RAR >3.5
- Post stenotic turbulence
- Absence of flow
Indirect Criteria for RAS
- Tardus Parvus renal hilum
- Renal asymmetry >2 cm
- Resistive Index >0.80 (Intrarenal)
- Delayed Acceleration time >0.07sec






Fibromuscular Dysplasia
- Angiopathy medium sized arteries
- Renal involvement 60-75%
- “String of beads/pearls” sign
- Affects Females 3-4:1 ratio usually of child bearing age



Sources:
Color Doppler sonography in the study of chronic ischemic nephropathy

Excellent! Thank you for putting this together. I have very little experience with this exam and it seems like it is always ordered on patient who weigh 300+ which makes it even more challenging to feel confident in preforming this exam.
LikeLike
Glad you liked it Leah!
LikeLike
[…] Read more -رابط المقالة […]
LikeLike
Amazing , very very helpful. Thank you .
LikeLiked by 1 person
You’re very welcome!
LikeLike
[…] Read more -رابط المقالة […]
LikeLike
Searched “Bruit Nutcracker” found this! Ive survived 15+ yrs, bp went from regular 120 to regular 210! Had all the Nutcracker symptoms.
At one point 12 yrs ago, had an EXTREAMLY loud abdominal/aortic/left side bruit at where the aorta goes off to kidney (per experts who heard it). They did many tests, they couldnt find the blockage, had other experts review tests, final explanation “youre a medical mystery”. Their Hypothesis, i had a fistula maybe hidden in my liver. HELP !
Recent CT notes enlarged left ovary vein and excessive vascular engourgment pelvic area. No one has a clue it may be this, please any suggestions while im still alive?
LikeLike
Oh wow!
LikeLike
You make things look so much easier to uderstand. Thank you for the iniative and your time.
LikeLike
Glad you found it useful!!!
LikeLike
This has been an amazing resource! I’ve been solely OB for over a decade but am getting back into the general/vascular game and this helps bring everything back. Thanks for all your hard work putting this together!
LikeLike
awesome!! thank you, I’m learning how to do renal dopplers on transplants at work , how you broke down the arcuate, interlobar , and segmental arteries is super helpful. =)
LikeLike
You’re welcome
LikeLike