

Thoracic ultrasound is used to image the lung, pleura and soft tissues. Lung ultrasound is particularly useful in critically ill patients and patients with infectious respiratory conditions like pneumonia.
Conditions Readily assessed with lung ultrasound:
- pleural effusion
- pneumonia
- pneumothorax
- pulmonary edema
Protocol
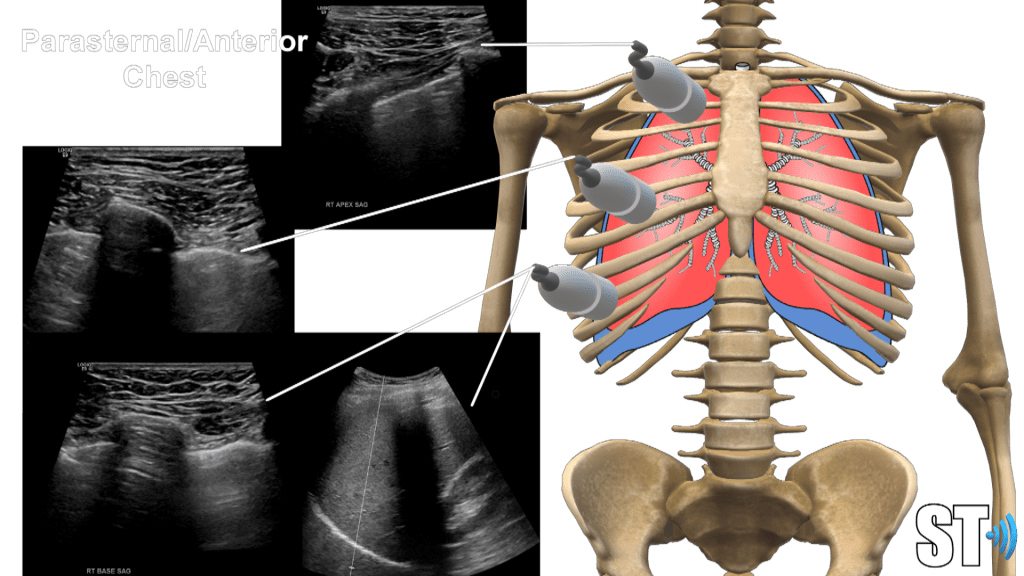
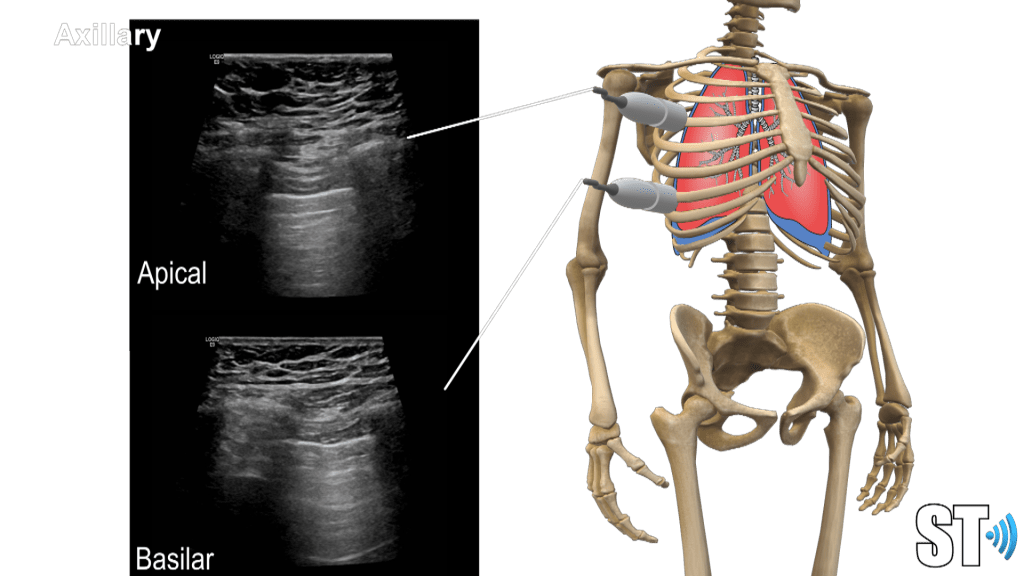
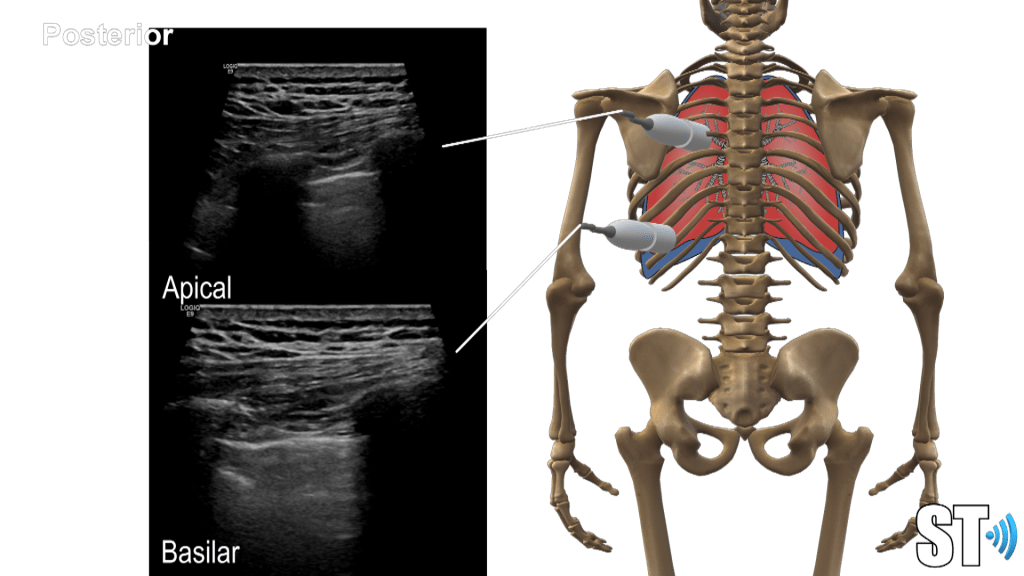
Using a linear, sector or small curvilnear transducer, divide the chest into parasternal, anterior and posterior axillary lines. Scan the basilar, mid and apical or upper portions of the chest. Scan the posterior aspect of the chest also at the base, mid and superior portions.
Anterior
Axillary
Posterior
You may scan the patient in supine, upright and prone positions (if intubated supine may be the only available scan approach).
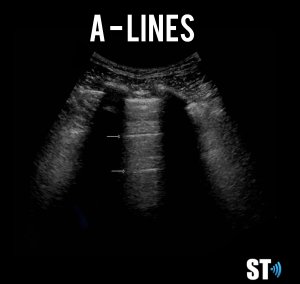
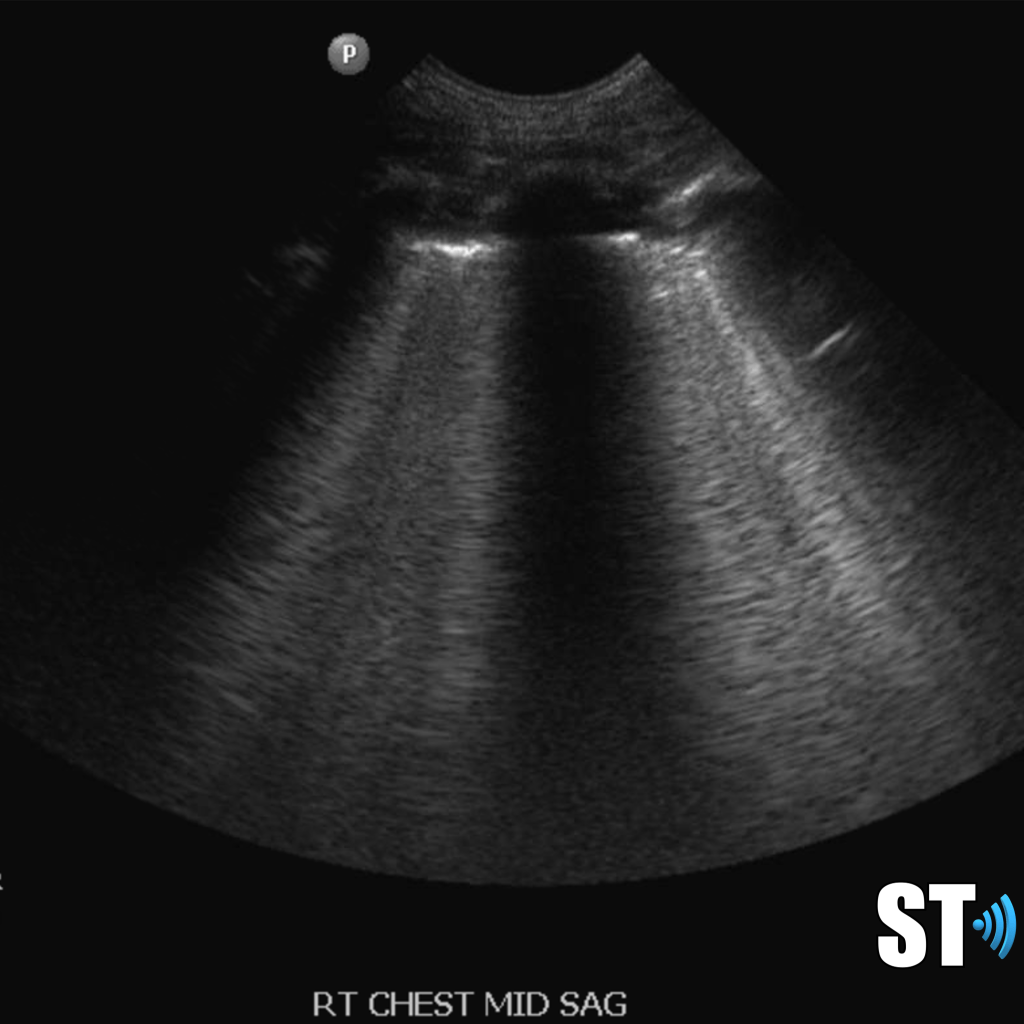
Normal lung ultrasound shows a clean linear pleural line with A-lines (multiple horizontal reverb artifacts) and lung sliding with respiration.

Imaging of lung movement can be stored as M-mode images or videoclips.
Lines and Signs
A-lines
Horizontal reverb artifacts at equidistant intervals from pleural interface.
B – lines
Vertical comet-tail reverb artifacts that extend to the bottom of the screen which may be normal (1-2 per intercostal space) or indicative of alveolar interstitial fluid (3 or more B- lines in multiple locations).

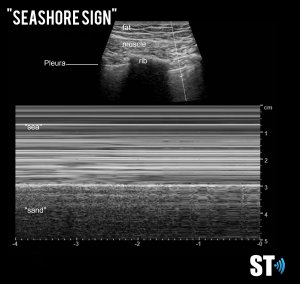
Seashore sign
Normal M-Mode sign where the “sea” represents the subcutaneous tissue and pleura and the “shore” represents movement of the lung field.
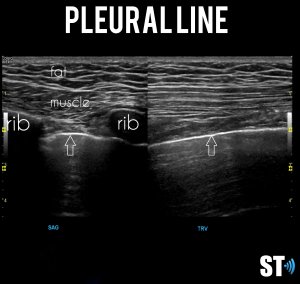
Pleural line
A thick pleural line may suggest a pneumonia, acute respiratory distress syndrome (ARDS), or fibrosis. An irregular line may represent fibrosis or pneumonia.
Lung point sign
A highly specific sign indicating pneumothorax. It involves visualizing the point where the visceral pleura begins to separate from the parietal pleural at the margin of a pneumothorax.
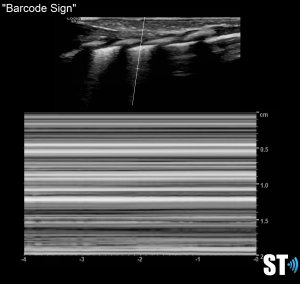
Barcode or stratosphere sign
Typically found in patients with pneumothorax. The lung sliding is absent and the sand-like appearance beneath the pleural line is replaced by parallel lines.
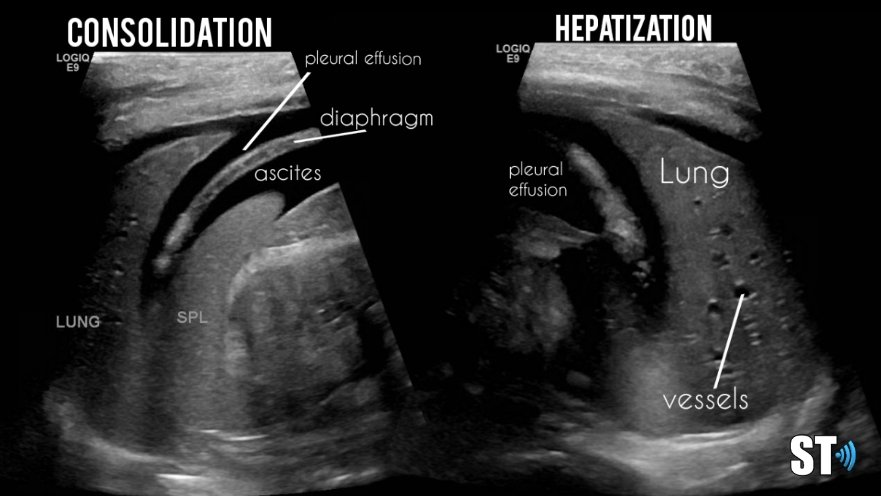
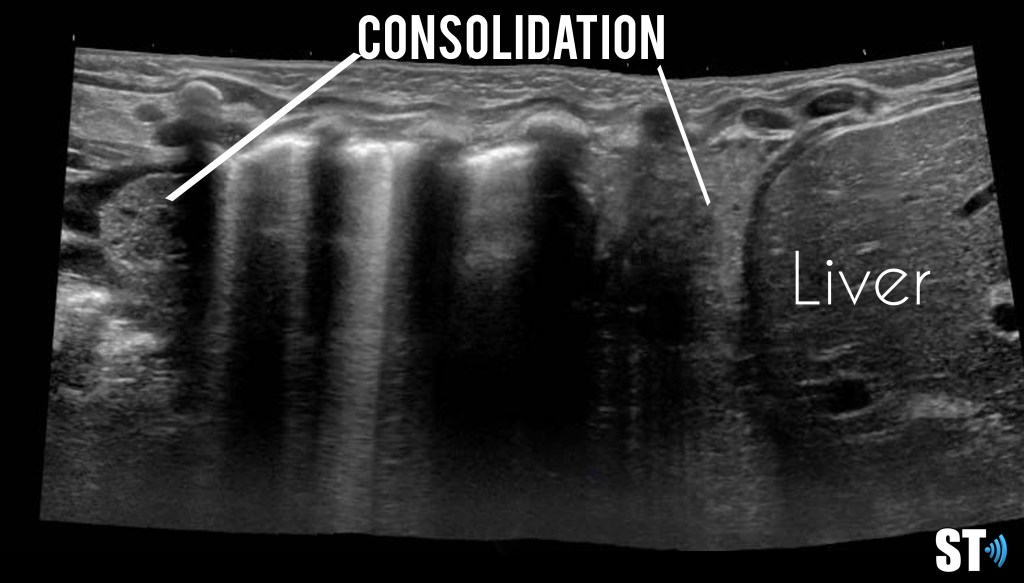
Consolidation
Hepatization of the lung parenchyma due to infiltration with fluid. May also have “air-bronchograms”.
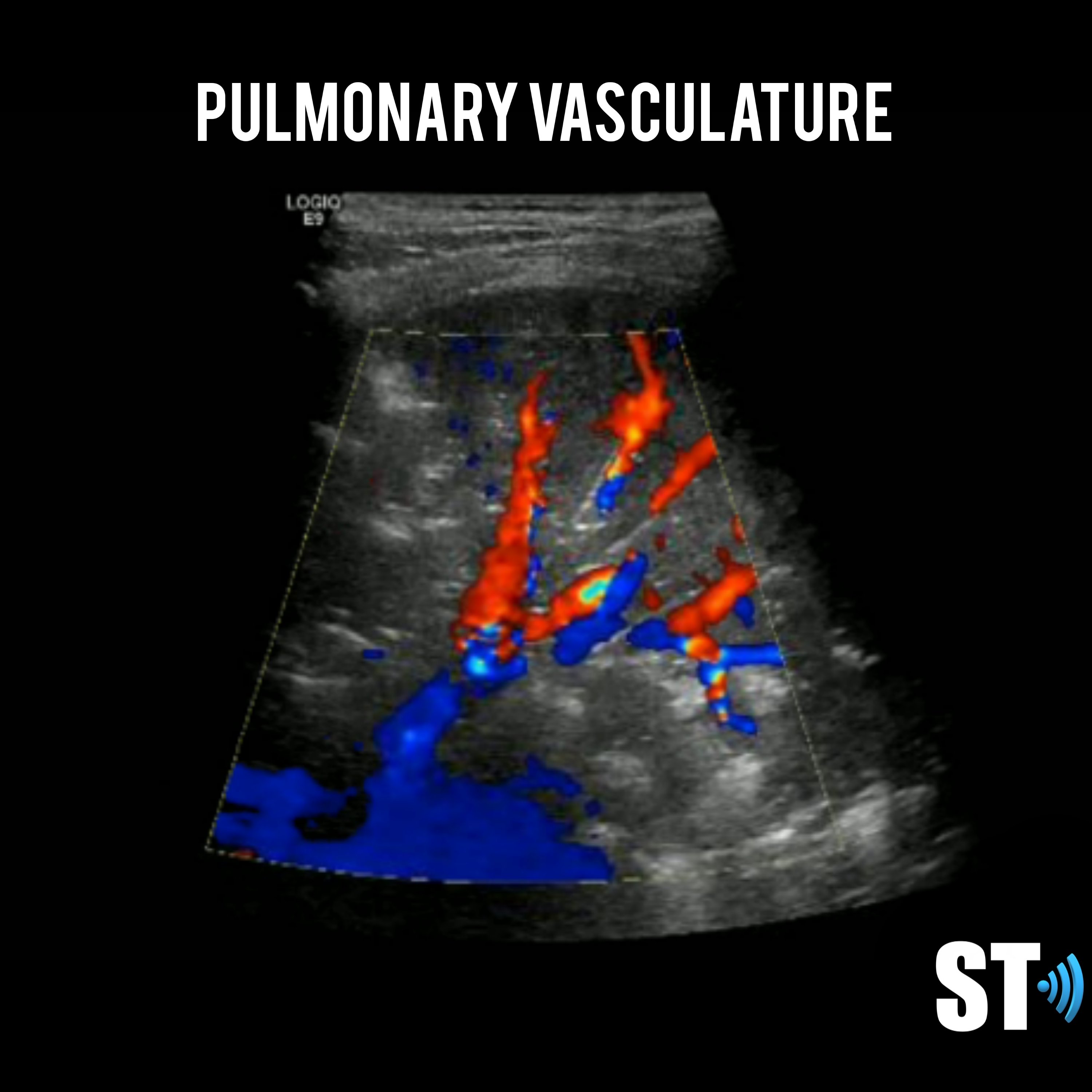
Color doppler will show blood flow through the pulmonary vasculature.
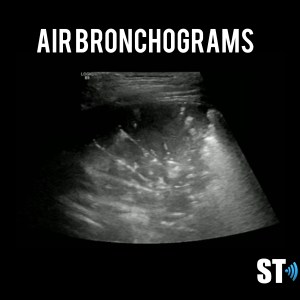
Air bronchograms
Dynamic or static air bubbles seen in the lung with consolidation and/or atelectasis.
Atelectasis
Complete or partial collapse of the entire lung or area (lobe) of the lung. Can be seen with consolidation.

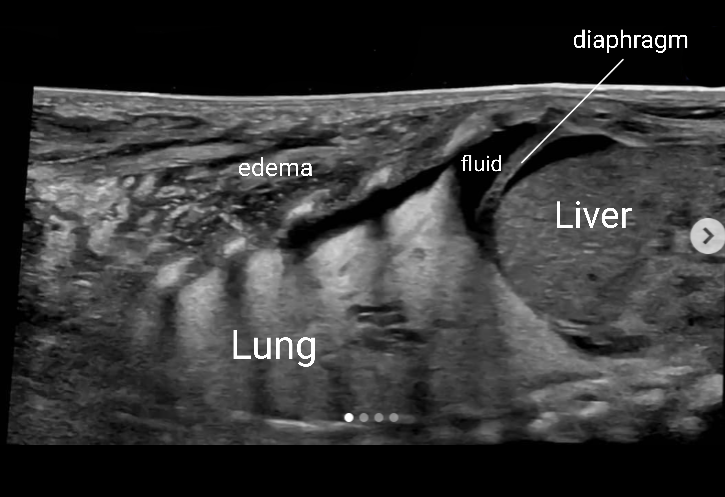
Pleural Effusion
Pleural effusion is a build up of fluid between the layers of the pleura. Scanning subcostally will show fluid above the diaphragm. Scanning intercostally will show fluid anterior the lung. Common causes for pleural effusion is infection, inflammation and malignancy.
The fluid can be anechoic or echogenic in cases of increased exudates, empyema, hemothorax and chylothorax (lymph collection). There may also be septations.
Pleural effusion can have transudative and exudative causes. Transudate is fluid pushed through the capillary due to high pressure within the capillary. Exudate is fluid that leaks around the cells of the capillaries caused by inflammation.
Transudate causes of pleural effusion
- Atelectasis
- Congestive heart failure
- Cirrhosis
- Hypoalbuminemia
- Peritoneal dialysis
- Pulmonary embolism
- Superior vena cava syndrome
Exudate causes of pleural effusion
- Infectious
- Bacterial infection
- Bronchiectasis
- Fungal infections
- Lung abscess
- Parasitic infections
- Tuberculosis
- Viral infection
- Malignancy
- Lymphoma
- Mesothelioma
- Primary lung cancer
- Pulmonary metastasis
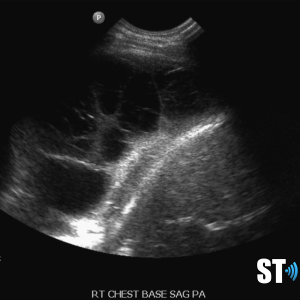
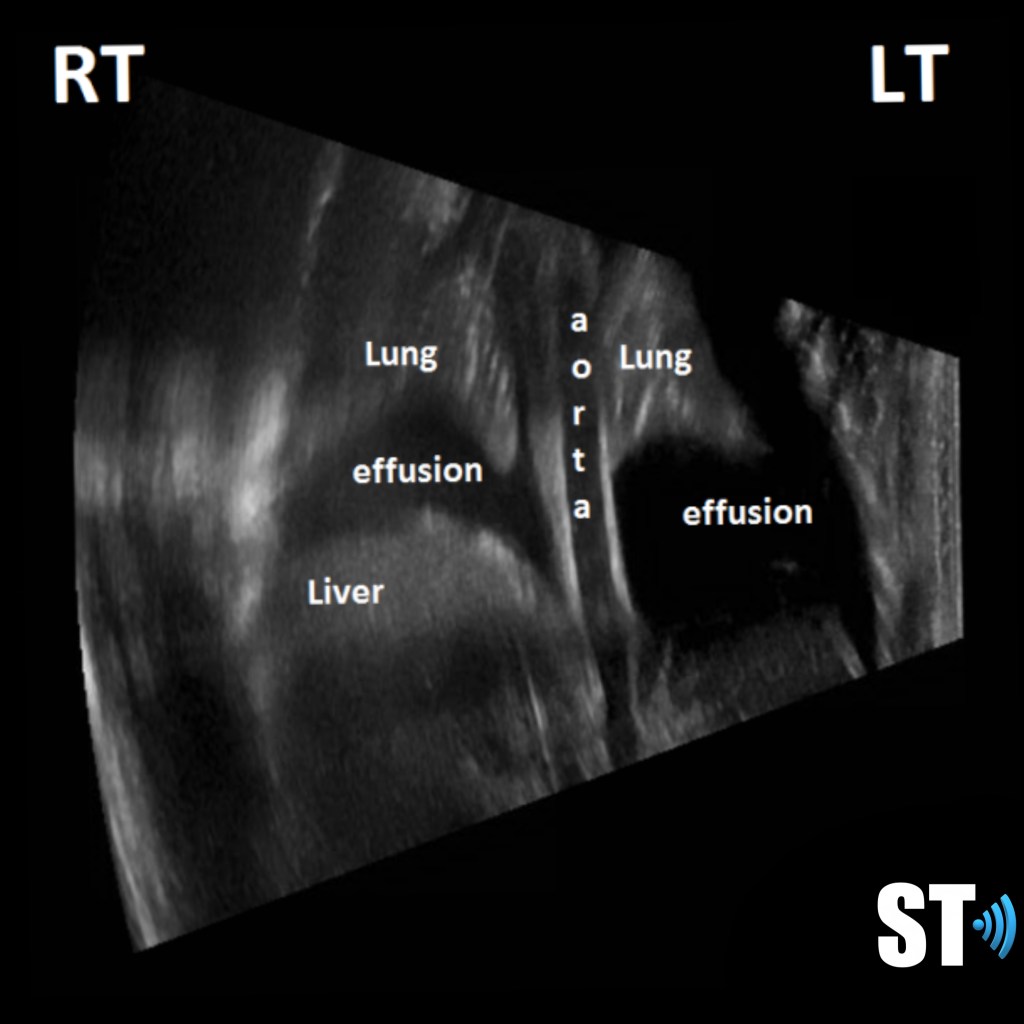
Moderate to large pleural effusion and pleural fluid anterior to lung

Large volume pleural effusion



Large volume echogenic pleural effusion
Large and or symptomatic pleural effusions may be treated with ultrasound guided thoracentesis which can double as a diagnostic procedure, where the fluid removed can be sent to pathology. Normal analysis of the fluid consists of cytology, chemistry and culture.
Loculated pleural effusion 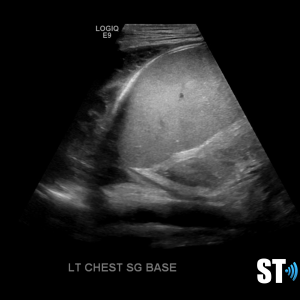
complex left pleural effusion

Pneumothorax
Ultrasound is more accurate in the diagnosis of pneumothorax that anterior posterior chest x-rays. Sonography will show lack of aerated lung by the absence of lung sliding and B-lines. A-lines will still be present as there is still air within the thorax and parietal pleura present. In the appropriate clinical scenario absence of lung sliding is diagnostic with pneumothorax with a 100% sensitivity and 96.5% specificity. [1]
Lung point is the junction between sliding lung and absent sliding is known as the lung point.
Consolidation/Atelectasis
In alveolar consolidation the lung parenchyma takes on the appearance of liver echotexture, “hepatization”. There may be air bronchograms present in consolidated tissue which appears as hyperechoic air bubbles with reverberation artifacts. Color doppler will show blood flow through the pulmonary vasculature.
Consolidation without air bronchograms
Consolidated lung 
Consolidated lung with collapse segment
Completely consolidated lung with pleural effusion and ascites
Consolidation with air bronchograms
Atelectasis can appear like consolidation but if air bronchograms are present they are usually static. The lung parenchyma will be compressed either in sections or globally.
Neonate with atelectasis and pleural effusion
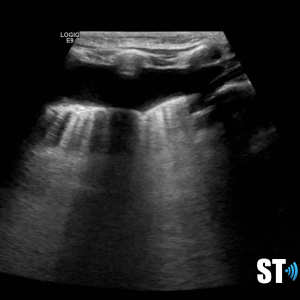
Alveolar Interstitial Pattern
This syndrome can be described as multiple B-lines in several scanning zones. In order to make the diagnosis you need at least 3 B-lines in any single intercostal space and in at least 2 zones.
B-lines 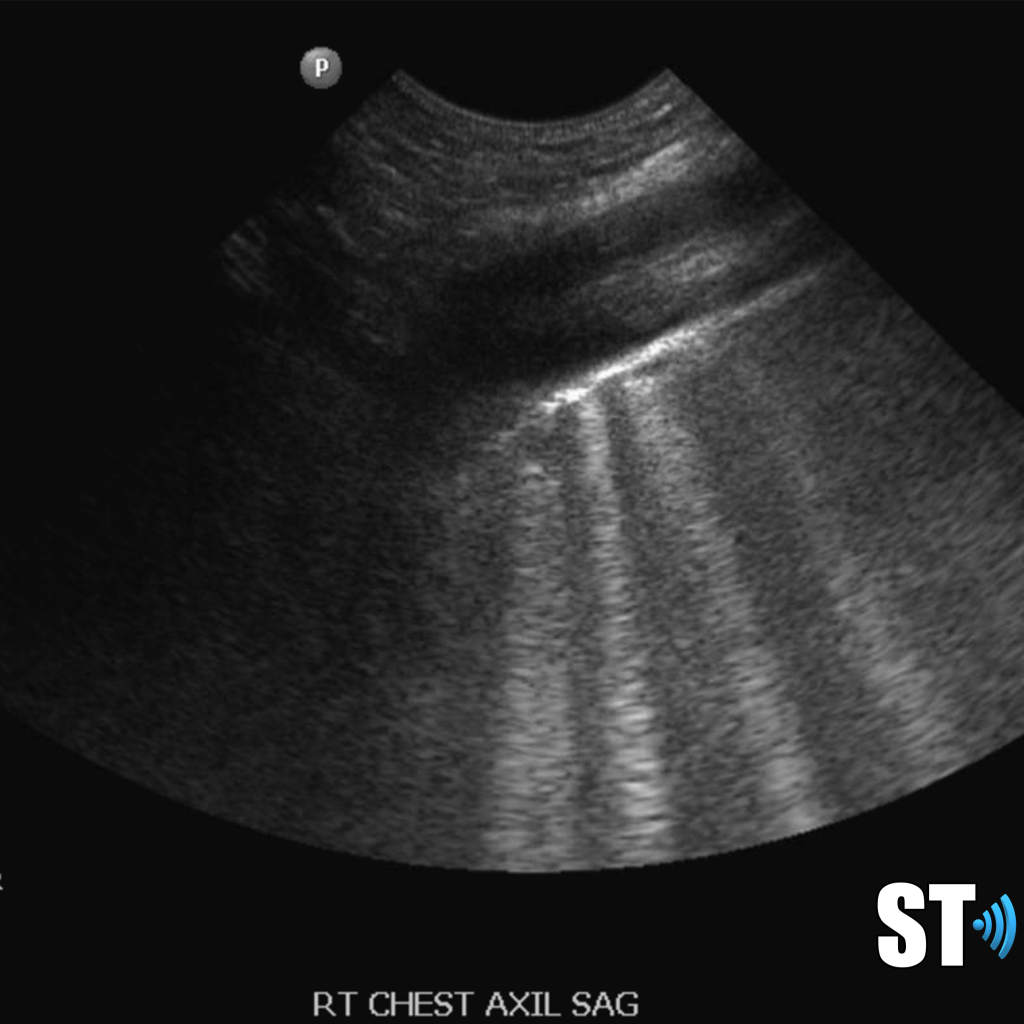
B-lines 
Pneumonia
Pneumonia is described as an infection of the lungs. It can be caused by bacteria and viral pathogens.
Early findings of pneumonia may be multiple B-lines and small areas of sub pleural consolidation. Further infection may lead to conslidations of larger parts of the lung and shred sign irregular consolidation with air interface.
Recent studies have reported that ultrasound is a valid modality in diagnosing pneumonia. [2],[3]In many cases it is being used in conjunction with radiography. Another study showed that pneumonia was missed in 5 of 76 children with pneumonia. [4]
Shred sign
Shred sign
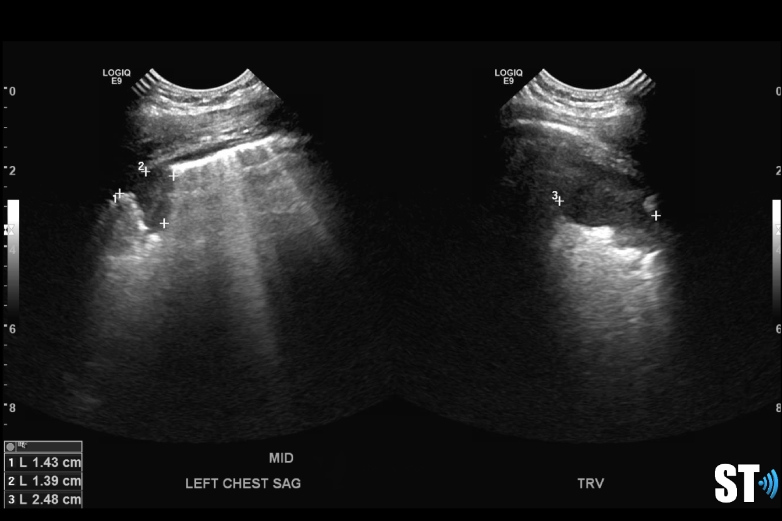
Heterogenous lung with pleural effusion in a patient with necrotizing pneumonia
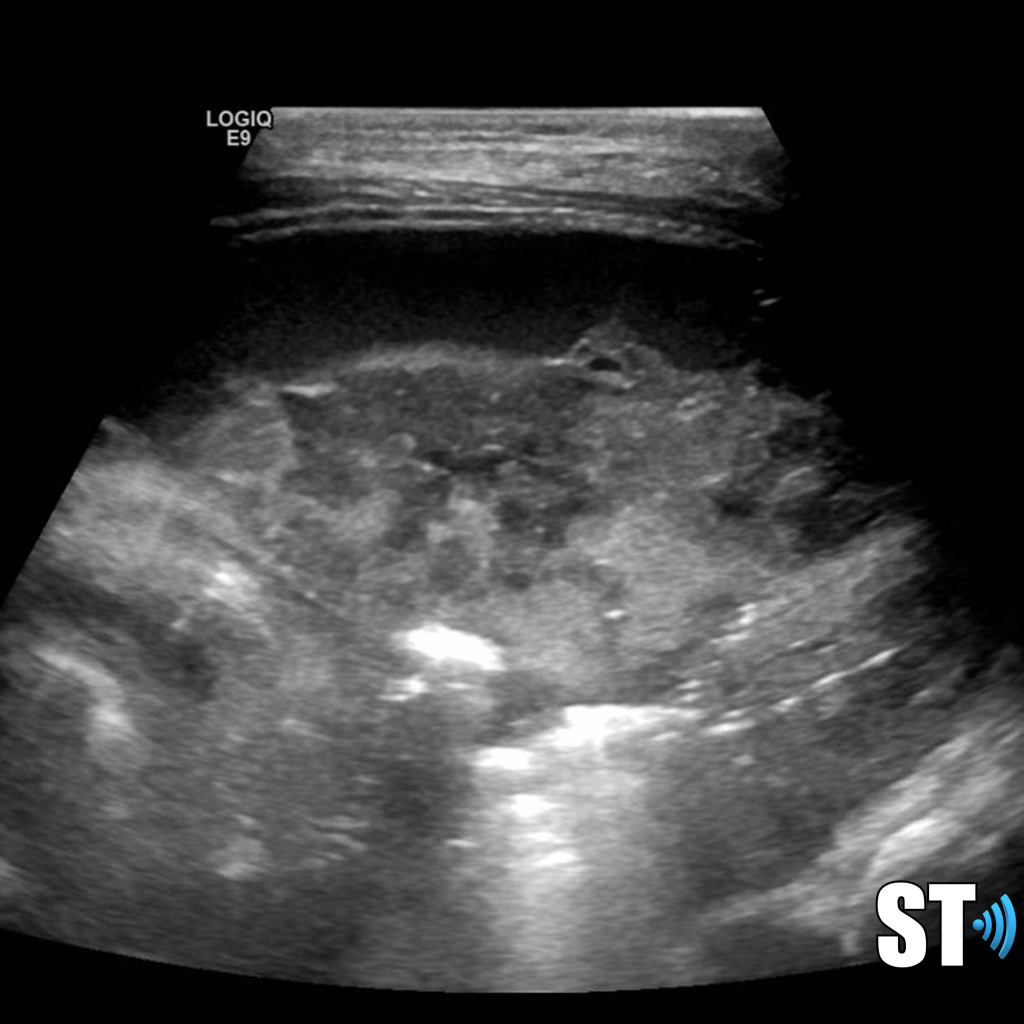
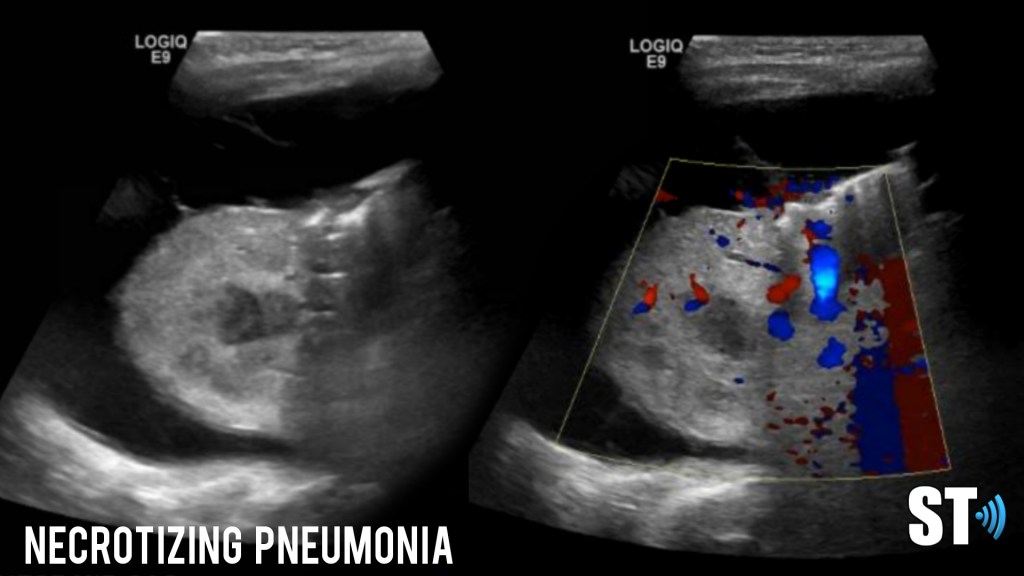
Necrotizing pneumonia
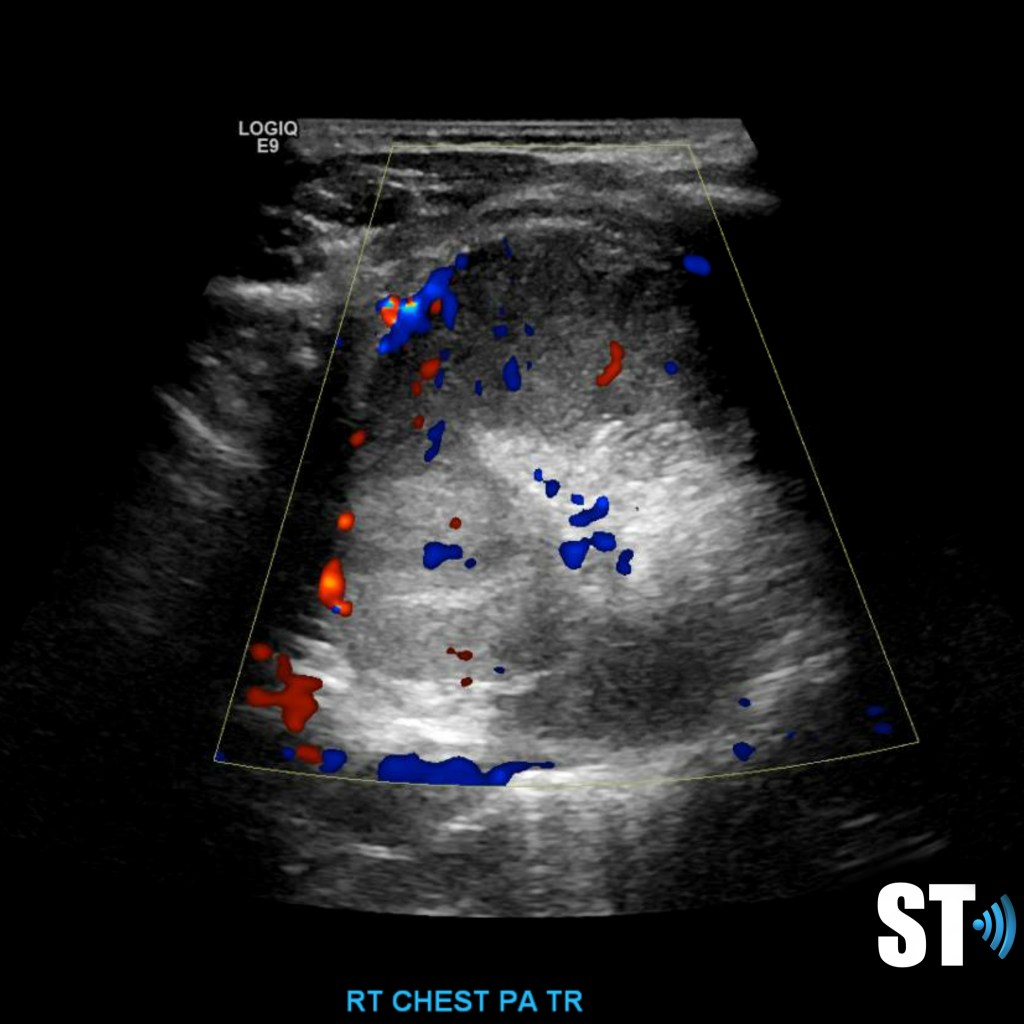
Malignancy
Lung cancer can lead to chest wall invasion which results in tumor growth on the pleura. Subpleural tumors can be due to metastatic processes as well. Parenchymal lung lesions can be appreciated if they are not obscured by air filled lung. In pediatrics primary tumors though rare can be pleuropulmonary blastoma, sacromas whereas metastatic tumors may be from osteosarcoma, Ewing’s sarcoma, Wilm’s tumors, hepatoblastoma and adenoid cystic carcinoma.
Right sided sarcoma with pleural effusion

Right chest sarcoma with pleural effusion 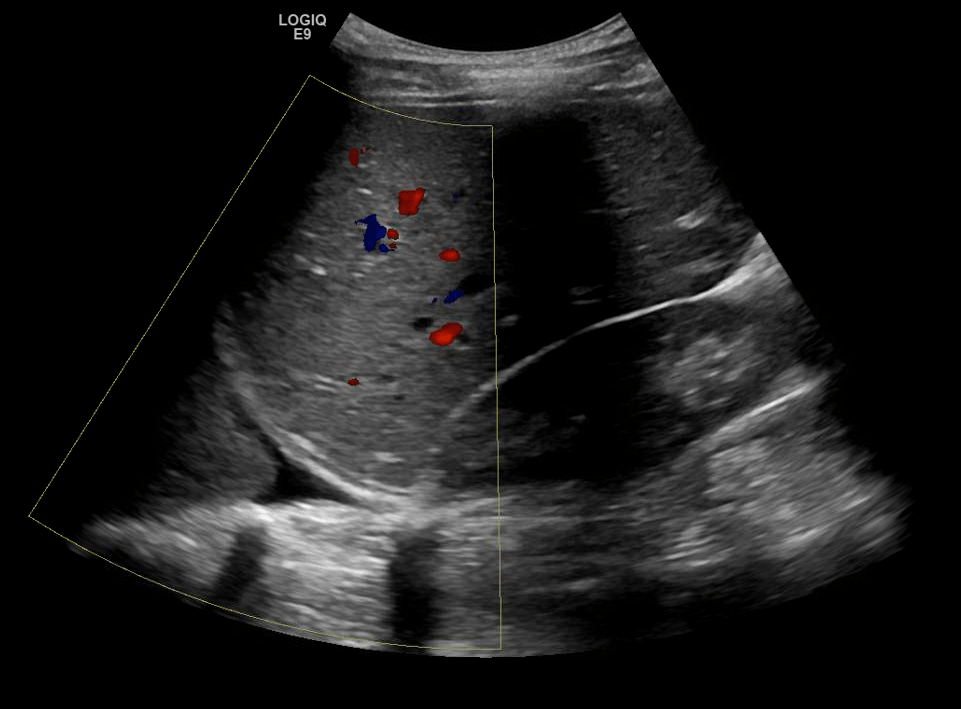

Pleuropulmonary blastoma
Primary chest neuroblastoma

Metastasis from osteosarcoma

Metastasis from rhabdomyosacroma
Diaphragmatic Hernia
Congenital diaphragmatic hernia is a defect or hole in the diaphragm that allows abdominal contents to enter the chest cavity. Most cases are diagnosed prenatally. Neonates typically present with respiratory distress acutely after birth. The lung on the affected side is usually hypoplastic.
Diapharagmatic hernias are usually classified by location.
- Location
- Posterolateral (Bochdalek)
- 80-90% of CDH
- 85% are left-sided, 10% right and 5% bilateral
- Anterior retrosternal or parasternal (Morgagni)
- 2% of all CDH
- Often asymptomatic in newborn period
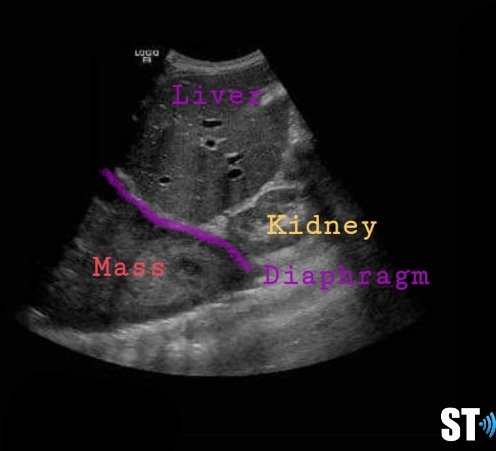
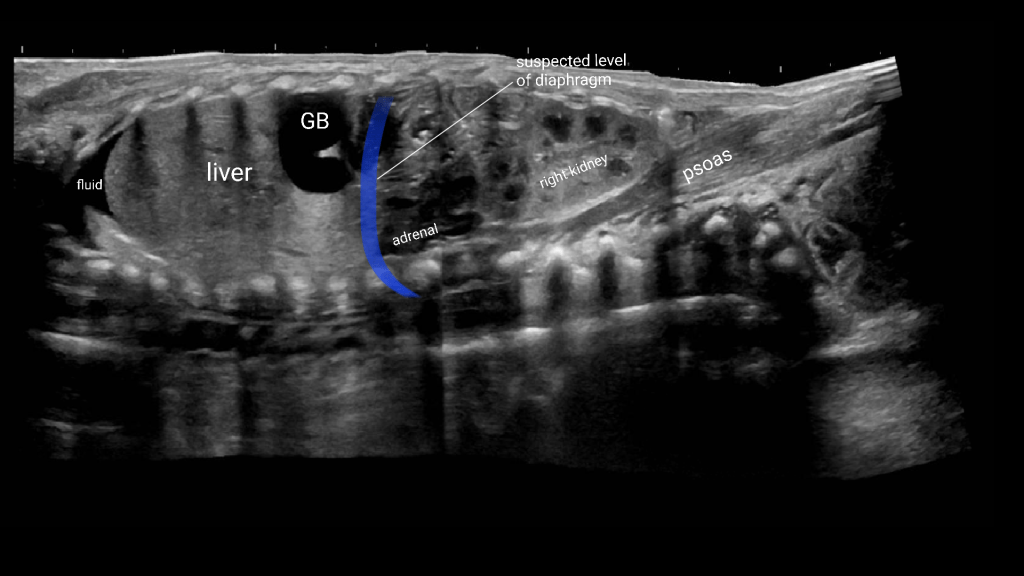
Right sided hernia with liver and hypoplastic lung

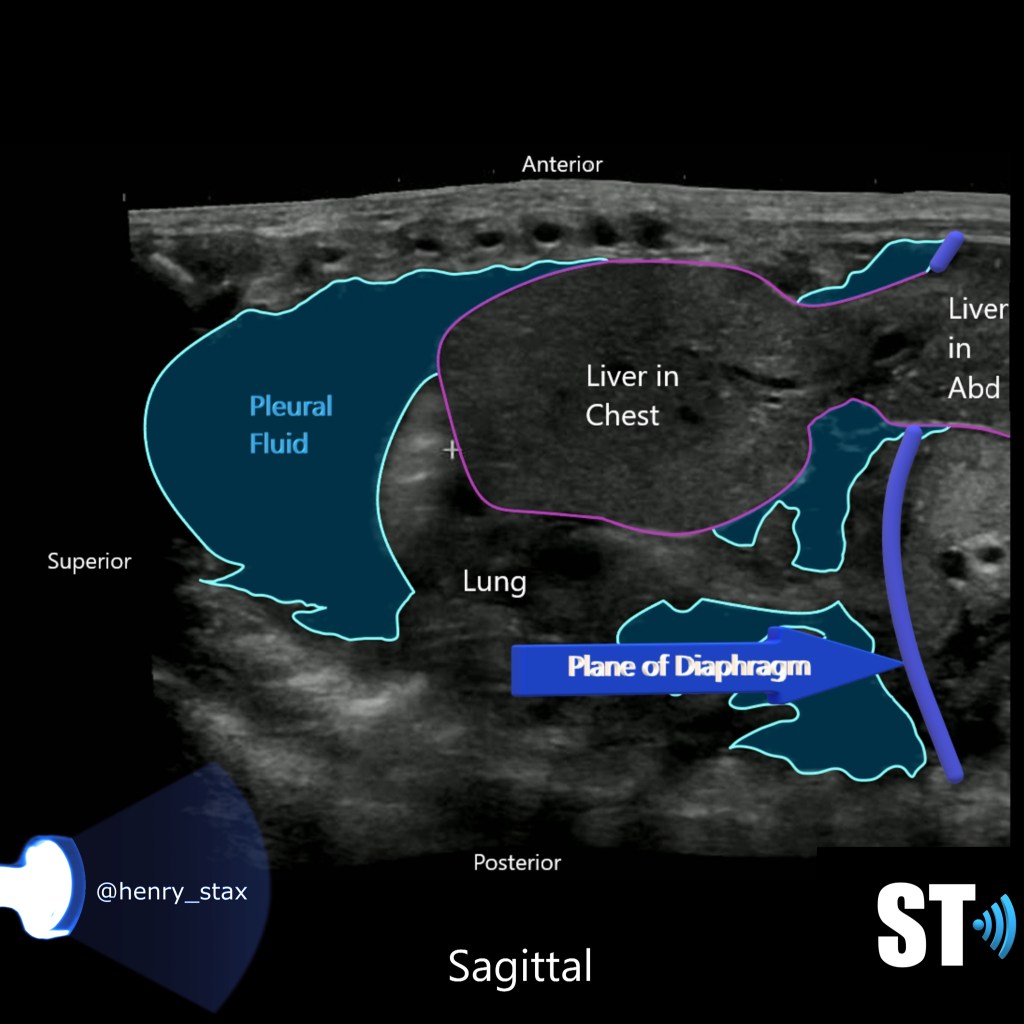
Liver and gallbladder in right chest
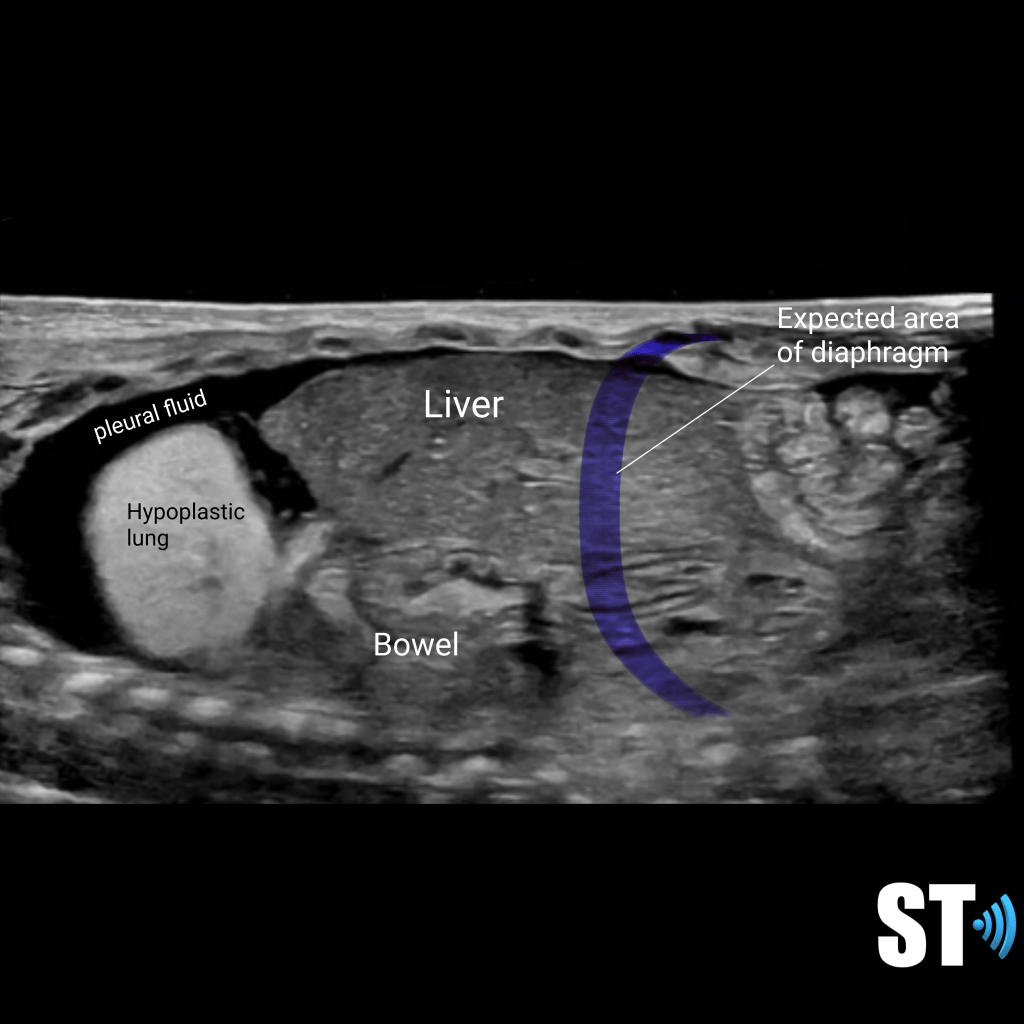

Diaphragmatic hernia with bowel
Sources:
1. https://www.ncbi.nlm.nih.gov/pubmed/20078434
2. Chavez, Miguel A, et al. “Lung Ultrasound for the Diagnosis of Pneumonia in Adults: A Systematic Review and Meta-Analysis.” Respiratory Research, vol. 15, no. 1, 2014, p. 50, 10.1186/1465-9921-15-50. Accessed 8 Nov. 2019.
3. Biagi, Carlotta, et al. “Lung Ultrasound for the Diagnosis of Pneumonia in Children with Acute Bronchiolitis.” BMC Pulmonary Medicine, vol. 18, no. 1, Dec. 2018, bmcpulmmed.biomedcentral.com/articles/10.1186/s12890-018-0750-1, 10.1186/s12890-018-0750-1. Accessed 29 Oct. 2019.
4. Urbankowska, Emilia, et al. “Lung Ultrasound in the Diagnosis and Monitoring of Community Acquired Pneumonia in Children.” Respiratory Medicine, vol. 109, no. 9, Sept. 2015, pp. 1207–1212, 10.1016/j.rmed.2015.06.011. Accessed 29 Oct. 2019.
Bibbo, Marluce, and David Wilbur. Comprehensive Cytopathology. 4th ed., 27 June 2014.
