

Eye Anatomy

The eye is a fluid filled orb that allows us to see things, like ultrasound images and beautiful trees and stuff! Here’s the anatomy that is pertinent for eye ultrasound.
- Cornea
- The cornea is the transparent anterior portion of the eye that covers the iris, pupil, and anterior chamber.
- Anterior Chamber
- The anterior chamber is the aqueous humor-filled space between the iris and the cornea.
- Pupil
- The pupil is a black hole located in the center of the iris which allows light to reach the retina.
- Iris
- The iris is the pigmented portion of the eye which contracts and dilates to control the amount of light that reaches the retina.
- Lens
- The lens is a transparent biconvex structure in the eye that, along with the cornea, helps to refract light to be focused on the retina.
- Vitreous Chamber/Humor
- The vitreous chamber is the cavity filled with clear gel (vitreous humor) between the lens and the retina of the eye.
- Retina
- The retina is the innermost, light-sensitive layer of tissue of the eye
- Sclera
- The sclera is the opaque, fibrous, protective, outer layer of the human eye containing mainly collagen and some crucial elastic fiber.
- Optic Nerve
- The optic nerve, also known as cranial nerve II, is a paired cranial nerve that transmits visual information from the retina to the brain.
- Central Retinal Artery
- The CRA is usually the first branch of the ophthalmic artery, arising as an independent branch or in common with one of the posterior ciliary arteries.
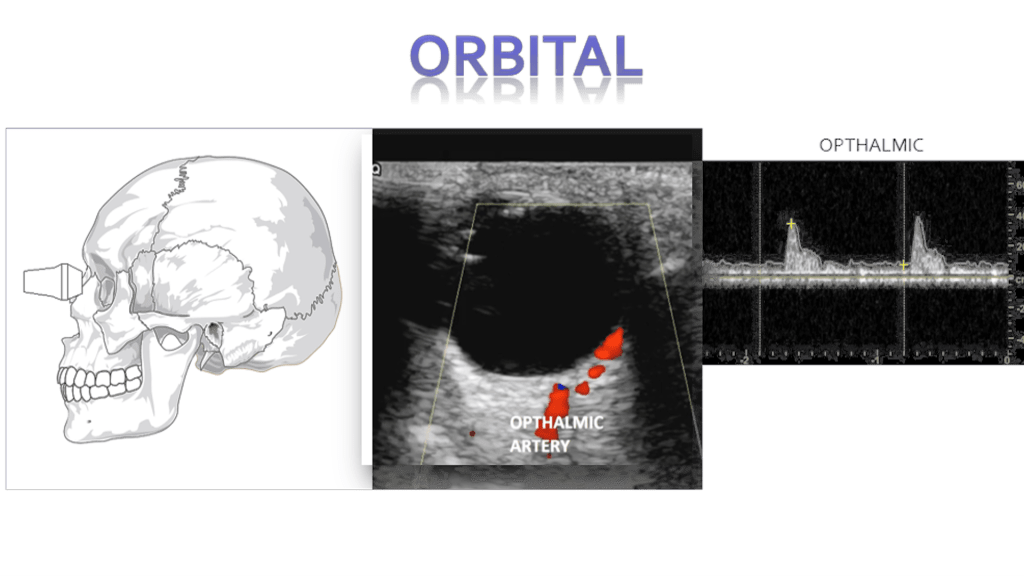
Technique

We scan the eye through a closed eyelid. Scanning in transverse and sagittal planes, making sweeping movements in all quadrants of the eye and also having the patient move their eyes side to side. Some practitioners like to use a lot of gel to give you space between the probe and the eyelid. I prefer to use less gel as in can get in the eye and cause mild irritation. Whenever possible try to use sterile gel. In some cases you can also use a Tegaderm patch over the eye but be cognizant that removing these can slightly pull on the eyelid and even remove false eyelashes in patients who are wearing them.
I like to use the GE 9L linear array transducer (or equivalent linear transducer from other manufacture), you can also use a higher frequency sector or microconvexed array. Larger transducers are not recommended as they are too big to fit in the orbital space, Even the 9L is difficult to use when scanning is sagittal.




Pupillary light reflex
The reflex is consensual: Normally light that is directed in one eye produces pupil constriction in both eyes…. The consensual response is the change in pupil size in the eye contralateral eye to to the one that is being illuminated. The clinical significance of this as it pertains to ultrasound is that it could be used when you want to evaluated but the eye is shut closed due to edema or other swelling.
Retinal Detachment
Peeling of the retina from its underlying support tissue (tethered to the optic nerve). On ultrasound you’ll see a thin echogenic serpiginous structure that sways with eye movement, this membrane is tethered to the optic nerve.
There are three different types of retinal detachment:
Rhegmatogenous
- Most common type
- Hole or tear that allows fluid to accumulate under the retina
- The detached retina loses blood supply leading to blindness
- Surgical emergency, as untreated detachment can lead to permanent blindness
Tractional
- Scar tissue forms on the retina which causes the retina to pull away
- Seen in patients with poorly controlled diabetes mellitus
Exudative
- Fluid accumulates but there’s no tear
- Macular degeneration, injury to the eye, tumors or inflammatory disorders
Retinal vs. Vitreous Detachment
Whereas in retinal detachment the retinal tissue will be attached or tethered to the optic nerve. Posterior vitreous detachment happens when the vitreous is detached from the retina. There will be a similar appearance but no tethering to the optic nerve will be present and the echogenic retinal lining will be seen still attached to the posterior wall.
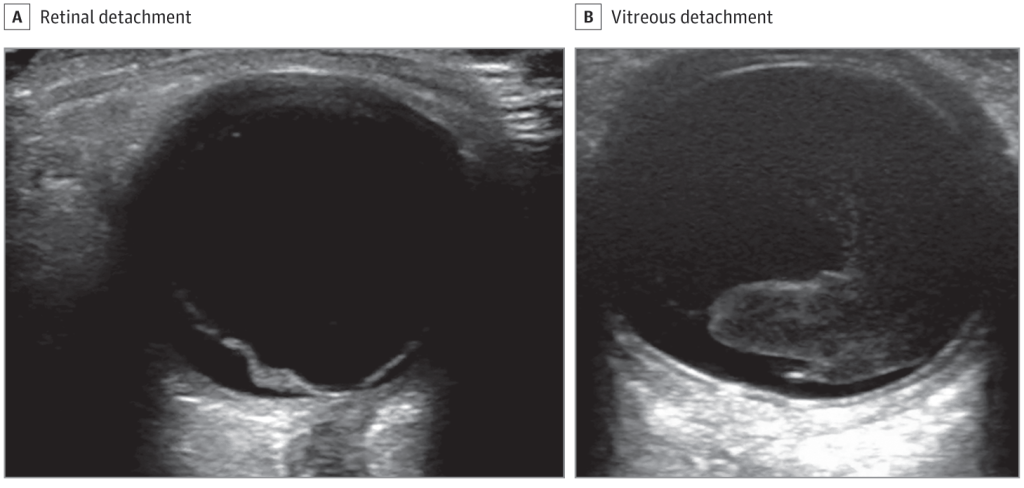
Retinal Detachment
Vitreous Hemorrhage
Any blood located in the vitreous chamber is a vitreous hemorrhage. Usual causes are proliferative diabetic retinopathy, posterior vitreous detachment, and ocular trauma. On ultrasound you’ll see a fluid fluid level within the vitreous chamber with the echogenic fluid representing blood, the echogenicity of the blood will vary depending on acuity (acute less echogenic, chronic more echogenic). The blood will also swish around with eye movements (washing machine sign)
- Diabetic retinopathy
- Trauma
- Retinal tear or detachment
- Posterior vitreous detachment
- Proliferative sickle cell retinopathy
- Age-related macular degeneration
Vitreous hemorrhage vs. Asteroid Hyalosis
Asteroid hyalosis is a degenerative condition of the vitreous with a prevalence of 1.2% in adults. It is found to be more frequent with aging, with 0.2% prevalence in 43- to 54-year-old and 2.9% in 75- to 86-year-old patients. It has been reported to mimic vitreous hemorrhage with the similar washing machine sing seen on ultrasound. On ultrasound there may be echogenic fluid with potential multiple echogenic foci.
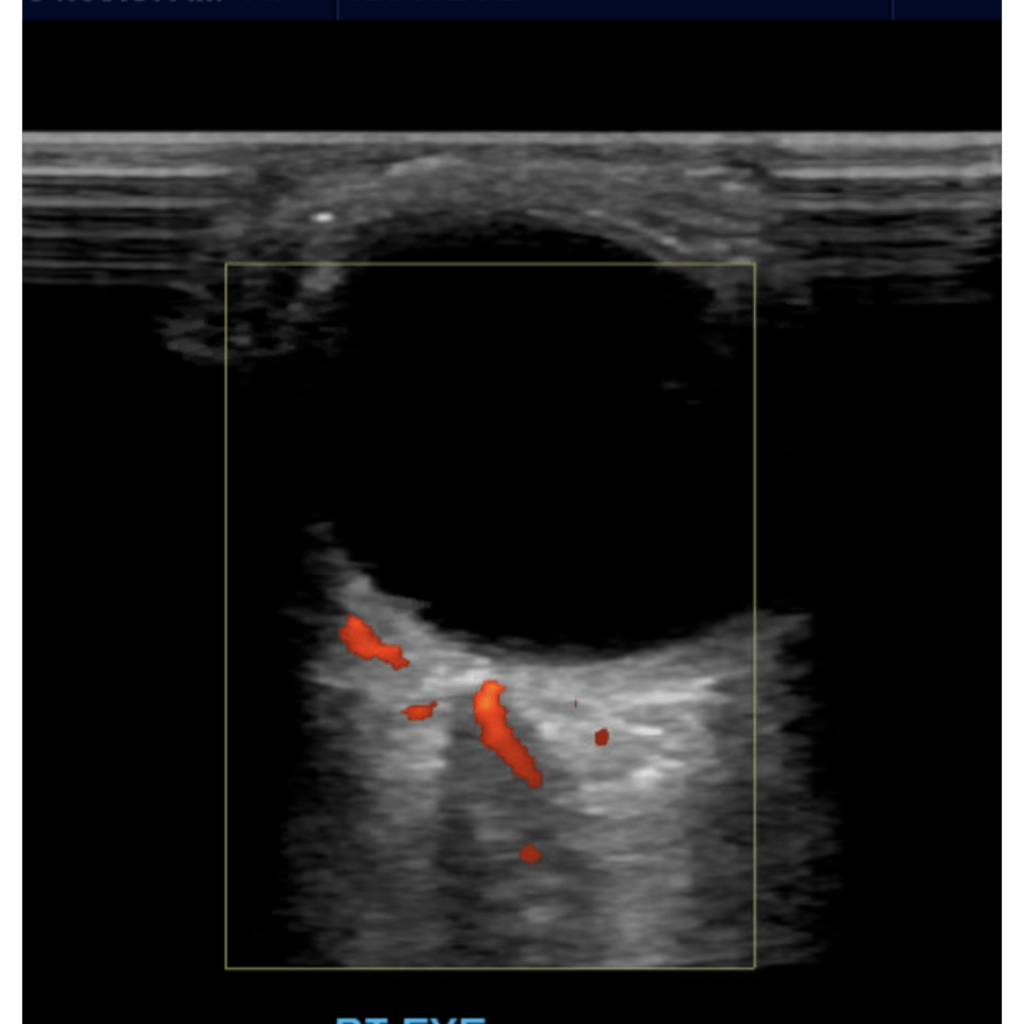
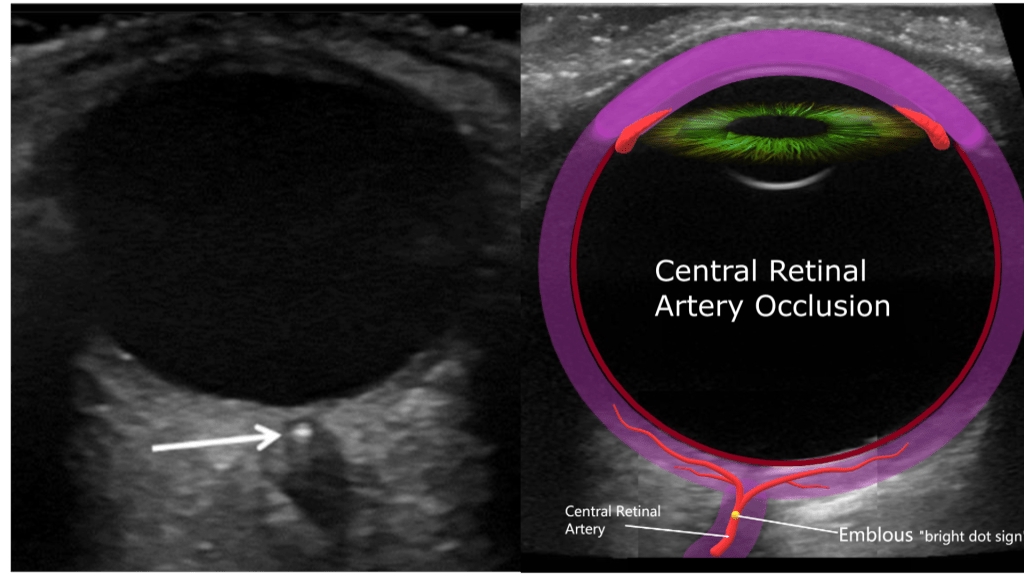
Central Retinal Artery Occlusion
Blockage of the central retinal artery usually due to an atherosclerotic thrombus (typically from an internal carotid artery plaque). Presents with sudden, painless, partial or complete monocular loss of vision. Also associated with giant cell arteritis. Patient describes “shade” or “curtain” coming down over entire visual field in the affected eye. Bilateral presentation is rare.
Sonographically you’ll encounter an echogenic foci posterior to the optic disc “bright dot sign” with lack of color or spectral flow distal to the thrombus
Increased Intracranial Pressure
Research has shown a correlation of increased ultrasound sheath diameter with increased intracranial pressure and papilledema. A prospective study of ICU and ED patients with invasive intracranial pressure monitoring found that an optic nerve sheath diameter of more than 5 mm correlated with intracranial pressure.
Proper measurement:
- 3mm from optic disc
- measure ONSD outer to outer, normally < 5mm
Normal Optic Nerve Sheath Diameter by Age
| Age Category (Years) | Normal ONSD Measurement |
| Adults (16+) | < 5 mm |
| Children (1-15) | < 4.5 mm |
| Children (<1) | < 4 mm |
Causes for increased intracranial pressure include:
- Intracranial hemorrhage
- Cerebral tumors
- Hydrocephalus
- Aneurysms
- Trauma
- Encephalitis
- Pseudotumor cerebri
Idiopathic intracranial hypertension aka pseudotumor cerebri is a condition characterized by increased intracranial pressure (pressure around the brain) without a detectable cause. The main symptoms are headache, vision problems, ringing in the ears, and shoulder pain. Complications may include vision loss.[2]

Lens Dislocation (ectopia lentis)
Lens dislocation (ectopia lentis) may occur after trauma or in association with ocular or systemic disease. Subluxation is the term used when the lens is partially dislocated but remains attached to the ciliary body Luxation is the term used when the lens is completely detached from the ciliary body. Luxated lenses may dislocate into either anterior or posterior chamber.
Sonographically the lens will be seen either free floating or in the dependent portion of the posterior chamber, or dislocated but still anchored by the ciliary body.

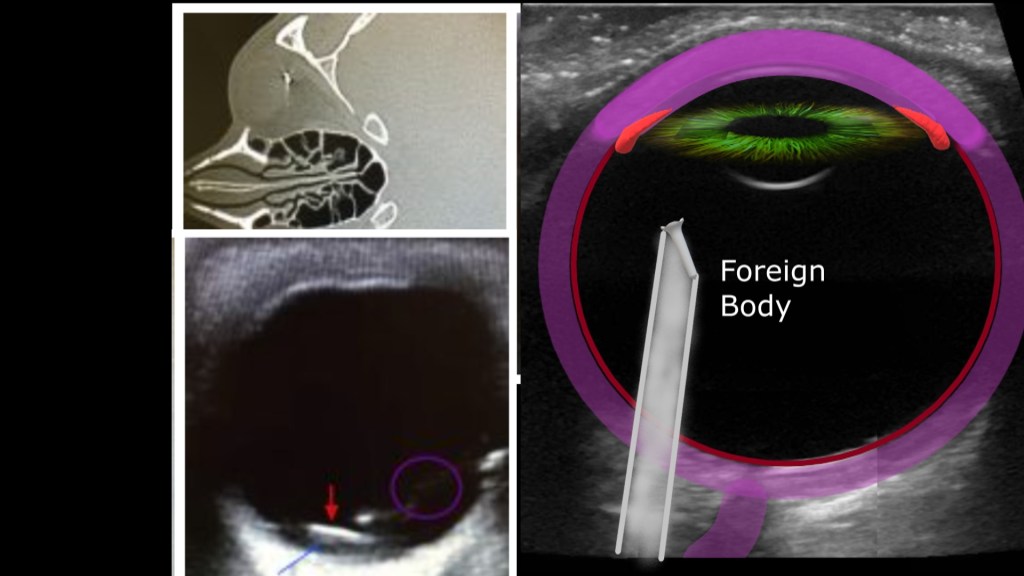
Foreign Body
IN the presence of ocular trauma with projectiles you may see an echogenic structure within the eye and depending on the material of the object you may see posterior artifacts.
Globe Rupture
Globe rupture often happens in the presence of blunt or penetrating trauma that causes a full thickness laceration or defect of the sclera. Traumatic globe rupture is an emergency.
These patients present with painful vision loss and extrusion of vitreous fluid.
As with rupture of other organs sonographically you may see a heterogenous amorphous complex structure with varying levels of echogenicity. The normal structures like anterior chamber, lens etc may not be easily identifiable. As with other traumatic injuries there may be significant edema or other inflammatory changes of the surrounding soft tissues.
Masses
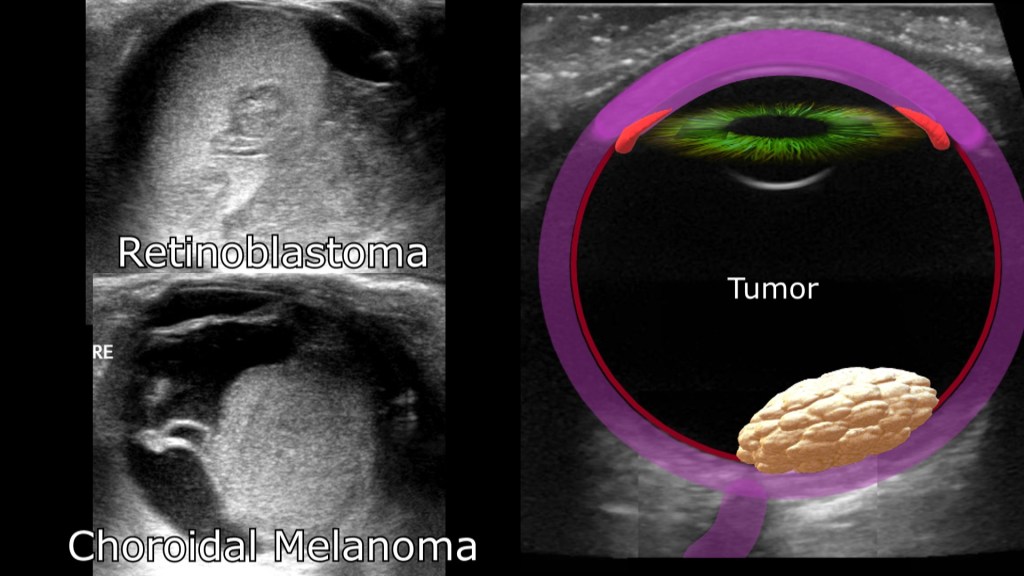
Intraocular Tumors
Ocular tumors range from benign to malignant, ultrasound can be used to identify the presence of, size and sonographic appearance (i.e. cystic, solid heterogenous) of the lesion.
Malignant
Ocular Melanoma
- most common ocular cancer
- starts in the pigment cells of the eye
- usually starts in the uvea/choroid
Retinoblastoma
- rare eye cancer seen in children
- develops from the immature nerve cells of the retina
- sometimes discovered incidentally on personal photos
- child may lose vision/need surgical removal of the affected eye
Primary Intraocular Lymphoma
- blood malignancy that develop from lymphocytes (eye is an uncommon location)
- eye lymphoma usually non Hodgkin’s type
- more common in elderly and immunocompromised patients
Metastatic
- cancer that has spread from primary site
- breast carcinoma.
- lung carcinoma.
- gastrointestinal tract carcinomas.
- genitourinary tract carcinomas.
- cutaneous melanoma.
- neuroblastoma.
Adnexal Cancer
- Neoplasms of the surrounding eye structures
- eyelids
- muscle
- tear glands
Benign
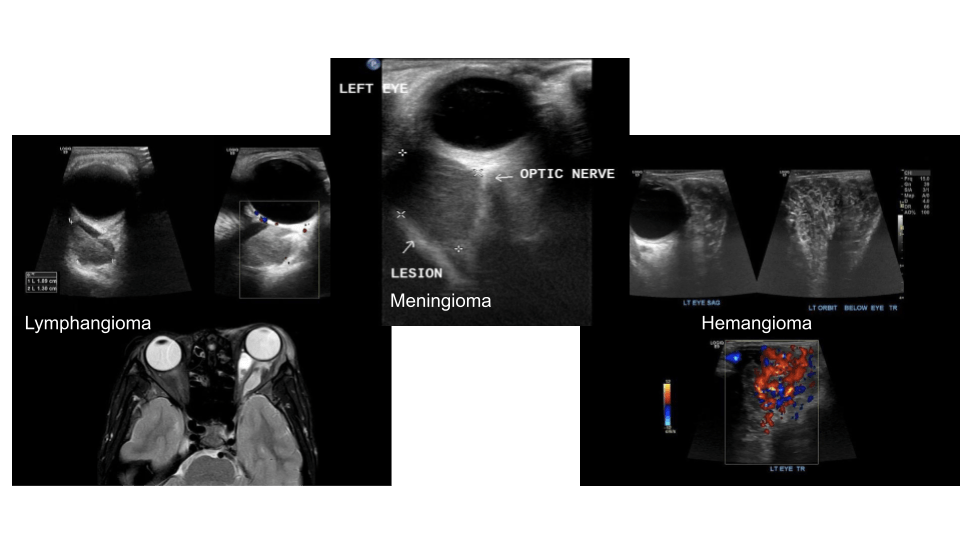
Benign intraocular tumors are non cancerous lesions like choroidal hemangioma, eye moles and cavernous hemangiomas and can be seen within or behind the eye.
Retro Orbital
Retorbital masses may be of hematogenous (i.e. from trauma) or lesions (benign/malignant)
Sonographically you’ll want to increase the depth to appreciate the posterior structures.
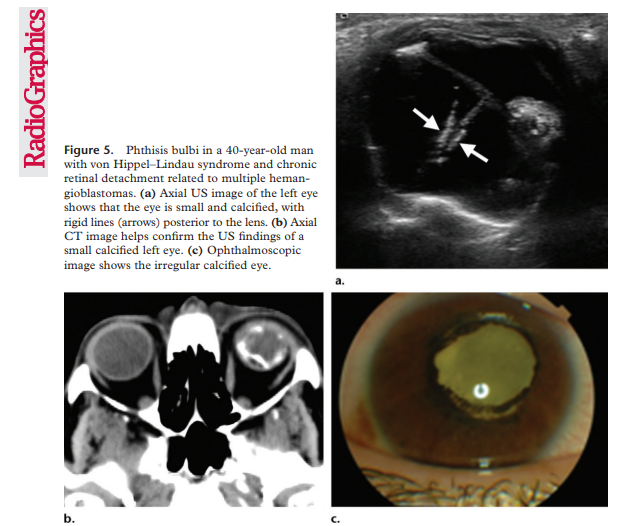
Phthisis bulbi
clinical condition representing end-stage ocular response to severe eye injury or disease damage, related to a variety of causes leading to scarring, inflammation, scaring, atrophy and eventually disorganization of the globe and intraocular contents. Also called end-stage eye, phthisis bulbi can be described as a shrunken, collapsed in form, non-functional eye and presents with a small squared off shape, opaque and thickened cornea, thickened sclera, neovascularization of iris, cataract, cyclitic membrane, ciliochoroidal detachment, and retinal detachment. A mnemonic rule used to describe phthisis bulbi is ”7S” referring to : Soft – Shrunken – Shapeless – Sightless – Structureless – Squared – Sore.
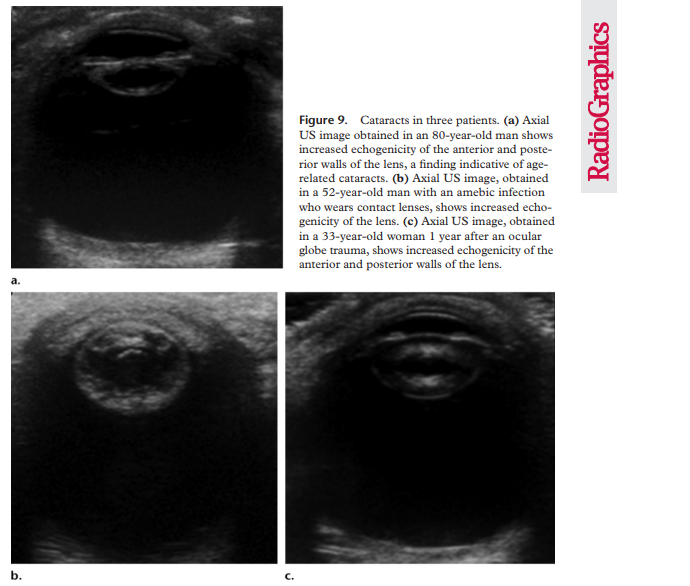
Cataract
When the lens becomes cloudy due to aging, trauma or radiation exposure this is referred to as a cataract. The normal lens on ultrasound echogenic at the edges and sonolucent everywhere else. On ultrasound a cataract can appear like irregular echoes or a heterogenous echotexture.
US of the Eye Made Easy: A Comprehensive How-to
Review with Ophthalmoscopic Correlation Rosa M. Lorente-Ramos, MD, PhD • Javier Azpeitia Armán, MD
Araceli Muñoz-Hernández, MD, PhD • José Manuel García Gómez, MD
Susana Bilbao de la Torre, MD
Asteroid Hyalosis: A Mimic of Vitreous Hemorrhage on Point of Care Ultrasound
Published online by Cambridge University Press: 30 August 2016
Charles E.A. Stringer, Justin S. Ahn and Daniel J. Kim
Kimberly H.H., Shah S., Marill K., Noble V.: Correlation of optic nerve sheath diameter with direct measurement of intracranial pressure. Acad Emerg Med 2008; 15: pp. 201-204.View In ArticleCross Reference
Efficacy of High Frequency Ultrasound in Localization and Characterization of Orbital Lesions
Rashmi M Nagaraju,corresponding author1 G Gurushankar,2 Bhimarao,3 and Bindushree Kadakola4
