

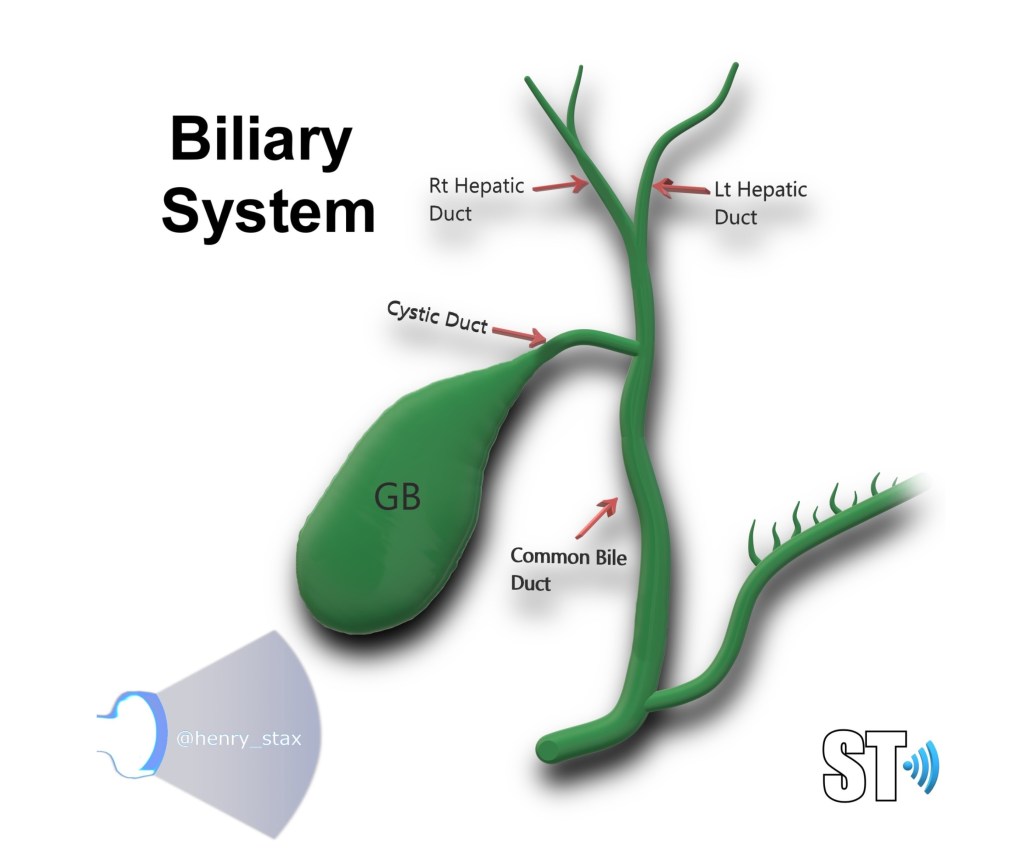
Choledochal cysts (CC) are rare congenital dilatation of the extra hepatic common bile duct (though they now include focal cystic dilatation of the intrahepatic bile ducts Caroli Disease), first described by Vater and Ezler in 1723. [1] Historically categorized into three types, choledochal cysts are now classified into five types known as Todani Classification. [2] CC is more common in females 4:1 and more common in Asian populations. [3]
Presentation
Choledochal cysts often present infants and young children within the first decade of life (Approximately 80%). [3] With infants presenting signs of obstructive jaundice and acholic stools with occasional palpable mass in the right upper abdomen if the lesion is large. If left untreated choledochal cysts can lead to pancreatitis. CC may also presents in adulthood with the most common symptom of epigastric or right upper quadrant pain which can progress to jaundice and cholangitis.
A classic triad of abdominal pain, jaundice, and a palpable right upper quadrant abdominal mass has been described in adults with CC but is found in only 10-20% of patients. The majority of patients only have one or two symptoms of the triad”.[3]
Imaging
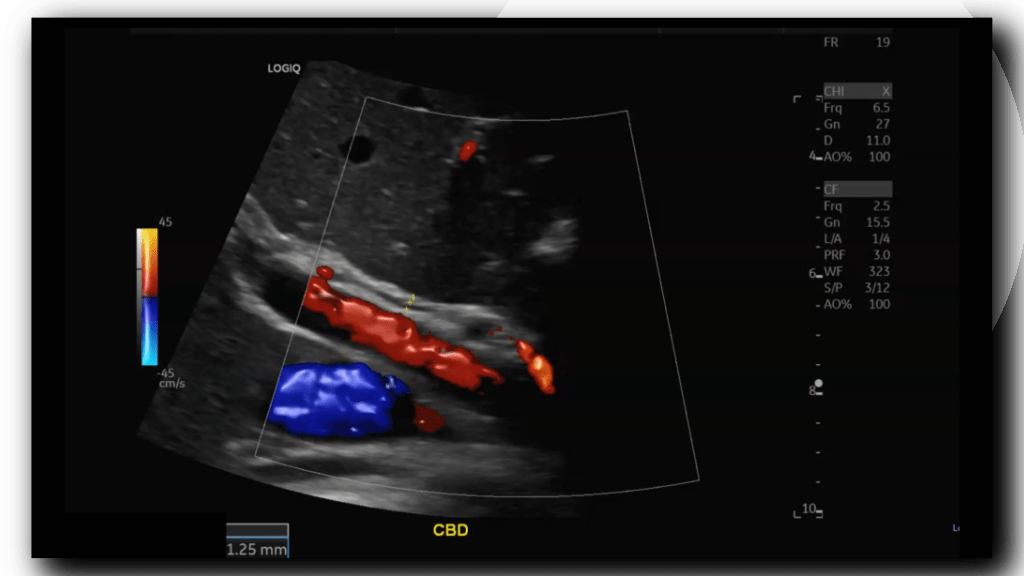
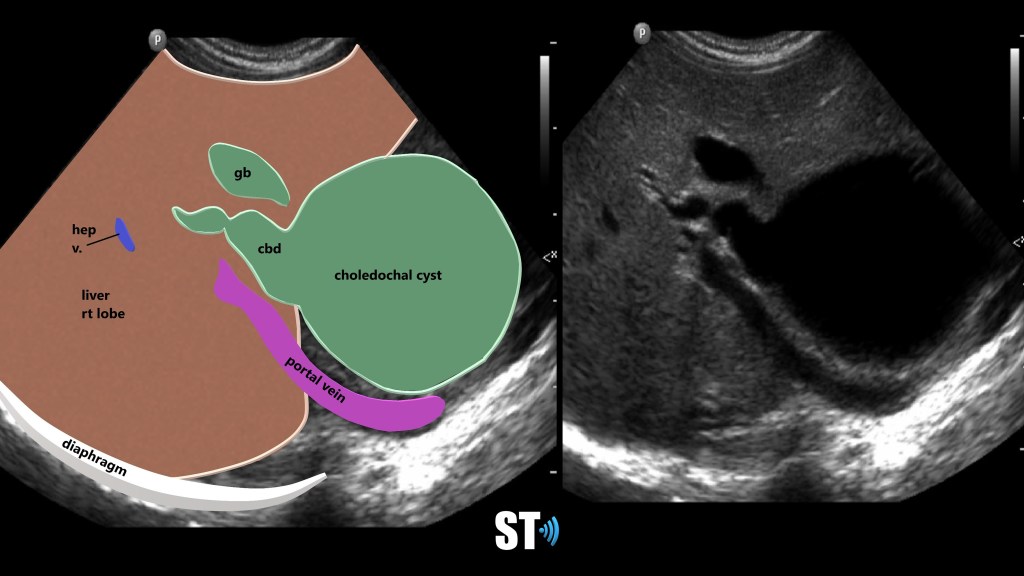
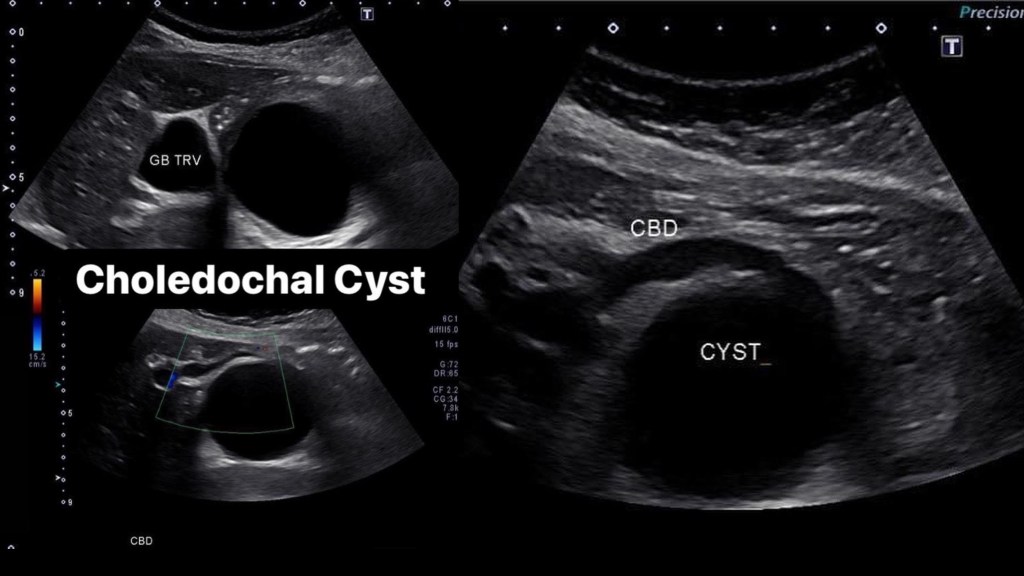
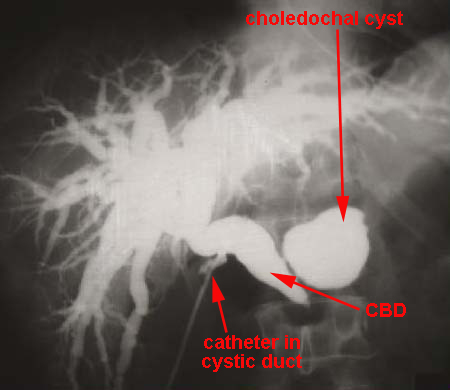
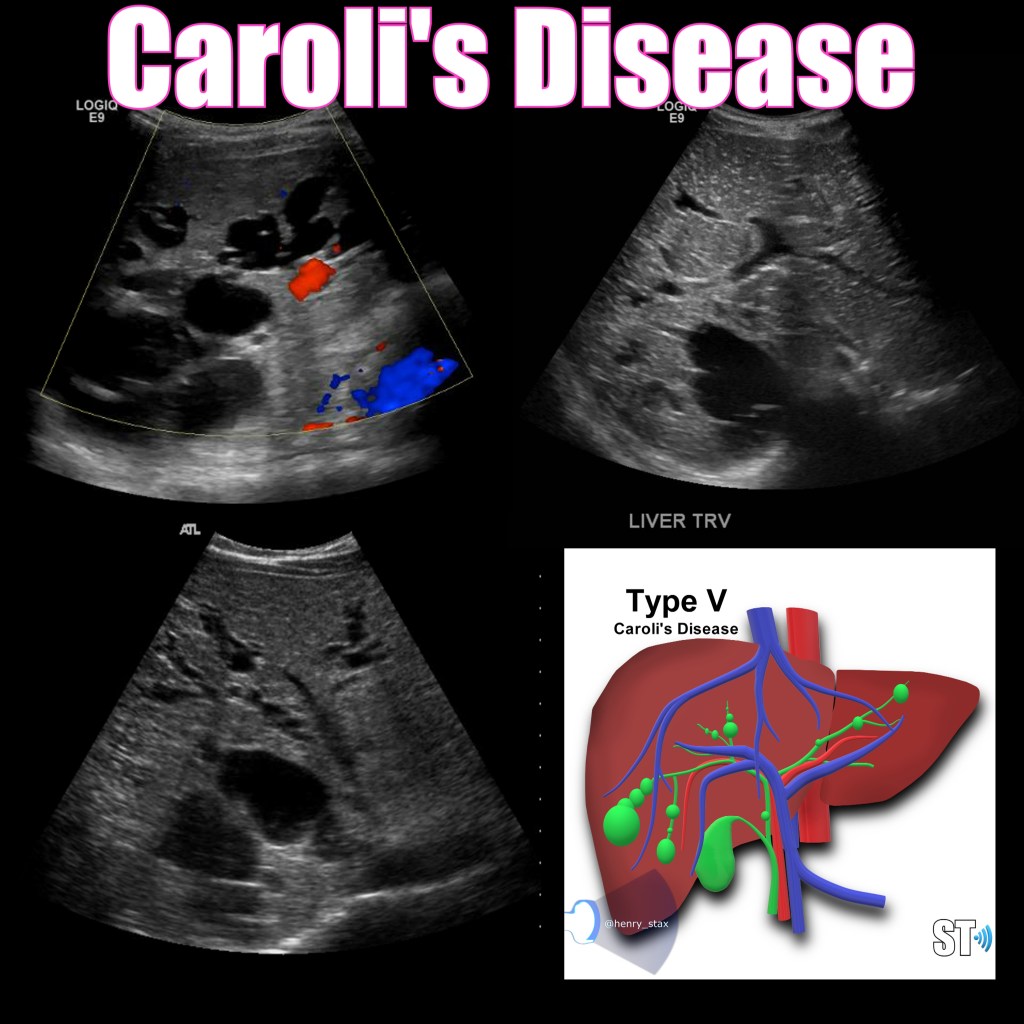
Choledochal cysts are routinely found on ultrasound in infancy, though they can be found on adults and fetal scans as shown below. An anechoic cyst will be present at or before the porta hepatis, size may be variable from small to quite large. In Caroli disease there will be innumerable intrahepatic cysts, this my be difficult to differentiate from polycystic kidney disease (ADPCKD) affecting the liver, typically ADPCKD cysts are non communicating. [3] Once found further imaging and work up must take place to properly classify and treat CC. Endoscopic Retrograde CholanigoPancreatography (ERCP) is the gold standard in diagnosing CC, however Magnetic Resonance CholangioPancreatography (MRCP) is now favored over ERCP due to its non-invasiveness and superior resolution. [5]
Case 1
Case 2

Todani Classification of Choledochal Cysts
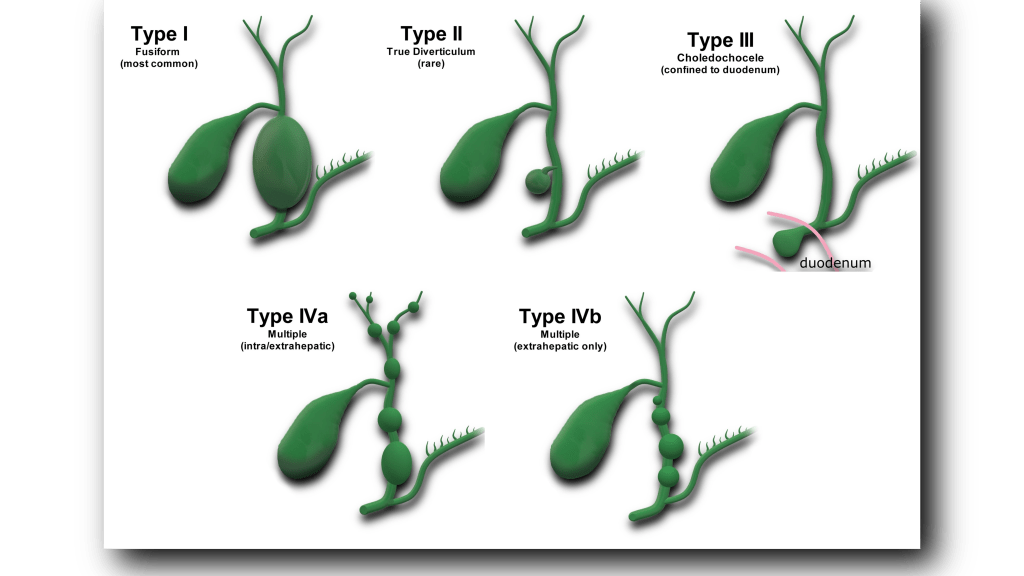
Commonly accepted classification developed by Todani et al. [2] Presented here are the five main types, with several subtypes.
- Type I: most common, accounting for 80-90% 1
- Type II: true diverticulum from extrahepatic bile duct
- Type III: dilatation of extrahepatic bile duct within the duodenal wall (choledochocele)
- Type IV: next most common
- IVa: cysts involving both intra and extrahepatic ducts
- IVb: multiple dilatations/cysts of extrahepatic ducts only
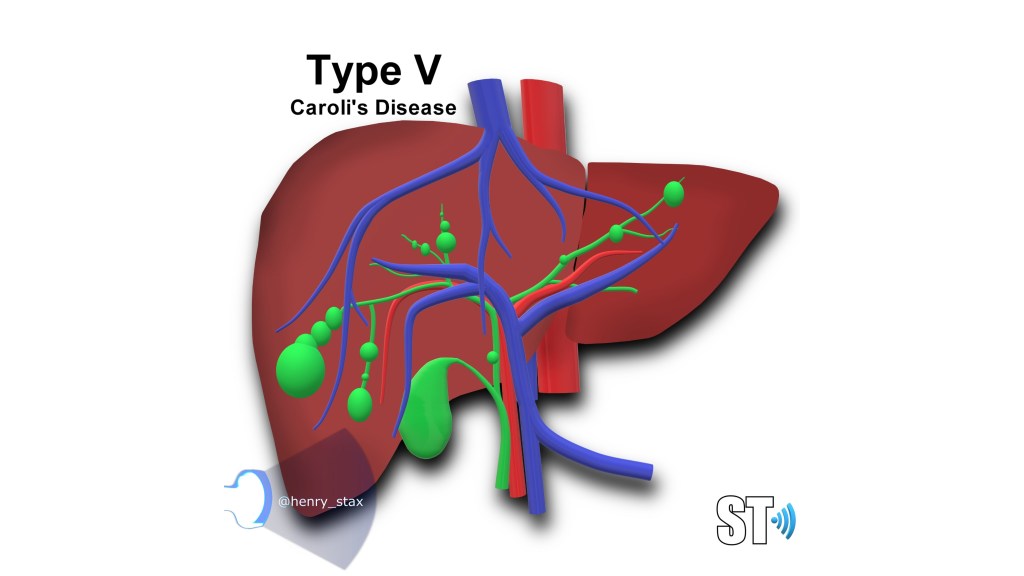
- Type V: multiple dilatations/cysts of intrahepatic ducts only (Caroli disease)
- Type VI: dilatation of cystic duct
Treatment
Excision of the CC has shown excellent results with an 89% event-free rate and an overall 5-year survival rate above 90%. Hence early diagnosis and appropriate management are needed for optimal results and good prognosis.
Bibliography:
- Vater A, Ezler C. Dissertatio de Scirrhis viserum occasione sections viri tymponite defunte. Wittenburgae Pamphlets. 1723;4:22
- Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K. Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg. 1977 Aug;134(2):263-9. doi: 10.1016/0002-9610(77)90359-2. PMID: 889044.
- Soares, K. C., Arnaoutakis, D. J., Kamel, I., Rastegar, N., Anders, R., Maithel, S., & Pawlik, T. M. (2014). Choledochal cysts: presentation, clinical differentiation, and management. Journal of the American College of Surgeons, 219(6), 1167–1180. https://doi.org/10.1016/j.jamcollsurg.2014.04.023
- Emily Tommolino, MD et. al. Choledochal Cysts Clinical Presentation https://emedicine.medscape.com/article/172099-clinical

My sister had that surgery, back 20 some years ago and still alive thanks to God and the surgeon !
LikeLike