


Neonatal-Infant Spinal Sonography
Spine ultrasound provides a high resolution imaging technique to rule out common and uncommon vertebral column pathologies like tethered cord syndrome and other spinal dysraphisms.
- Midline or paramedian masses
- Midline skin discolorations
- Skin tags
- Hair tufts
- Hemangiomas
- Small midline dimples
- Paramedian deep dimples



Preparation
Make sure infant is well fed to reduce fussiness and potential crying, use warm gel and lay the patient prone with small towel roll under umbilicus to arch back.
Anatomy

The vertebral column is divided into 4 segments; A cervical portion which is the most cephalad and located in the neck contains 7 bones labeled C-1 through C-7. The second segment is the thoracic vertebrae, it is the largest segment just below the neck located in the chest and contains 12 bones. Inferior to this is the lumbar vertebrae which contains 5 bones that are quite broad in comparison. Lastly is the sacrum, a large triangular bone at the base of the spine. It is formed by the fusing of sacral vertebrae S1–S5.

Finding the Conus
You can either count from the sacrococcygeal area there will be 5 sacral and 5 lumbar vertebrae, the conus medullaris should end at of before L2. Another method is to use the last rib, while scanning int the lumbo-thoracic region angle laterally and you will encounter echogenic spherical structures that are the ribs. Find the last rib, this should be your the 12th rib associated with T12. L1 and L2 should follow caudally. A potential pitfall with this method is that some people have 11 or 13 pairs of ribs, which is why both methods should be used to improve accuracy.

Variants
Mild Dilatation of the Central Canal
A slight dilatation of the spinal cord’s central canal is sometimes observed in newborns. It is an incidental finding considered to be a normal variant and of no clinical significance. It is not to be mistaken for a syrinx.
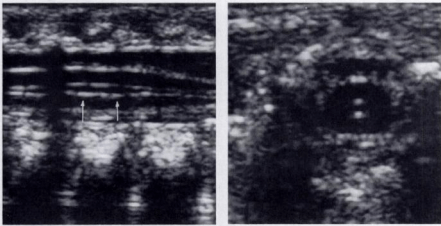
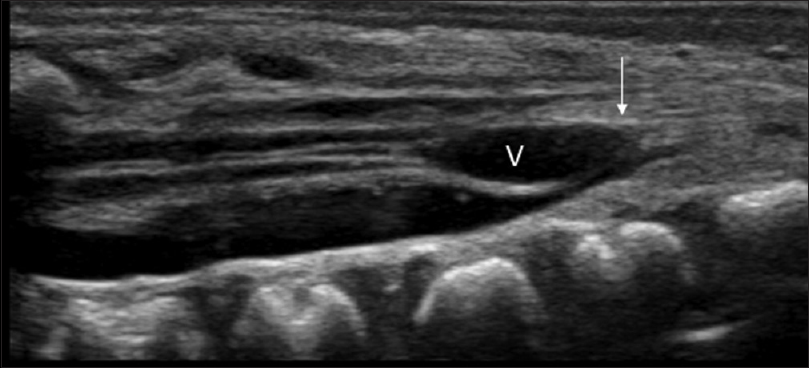
Ventriculus Terminalis
The ventriculus terminalis is a small, ependyma-lined, oval, cystic structure positioned at the transition from the tip of the conus medullaris to the origin of the filum terminale. The ventriculus terminalis develops during embryogenesis as a result of canalization and retrogressive differentiation of the caudal end of the developing spinal cord and regresses in size during the first weeks after birth . This variant causes no clinical symptoms.
Filar Cyst
This is a cystic structure that is routinely seen within the substance of the Filum. Also of no clinical significance.

Tethered Cord
Tethered cord is a syndrome with several causes in which the spinal cord is pulled tight due to a mass or dysraphism like spina bifida.
The normal spinal cord moves freely within the spinal fluid filled canal. When there is tethering, the cord can be taut and attached to the vertebral column or subcutaneous tissues by a thickened filum terminale, dermal sinus tract, diastematomyelia (split cord), or a lipoma.
When this is present the conus medullaris will be located below L2, it can be located at L4 and even lower in more severe cases.




Caudal Regression Syndrome aka sacral agenesis or hyperplasia is a rare birth defect occuring in 1-25,0000 births. In this image you can see an almost absent sacral area with a blunted conus medularis.

Caudal regression syndrome 
Single dysplastic sacral element
Spina Bifida the 3 most common types of spina bifida is meningocele, myelomeningocele and spina bifida occulta.
Meningocele

Sacral Meningocystocele





Sources:
Lisa H. Lowe et. al. American Journal of Roentgenology. 2007;188: 733-738. 10.2214/AJR.05.2159
Karin, Unsinn M. et. al. “US of the Spinal Cord in Newborns: Spectrum of Normal Findings, Variants, Congenital Anomalies, and Acquired Diseases.” US of the Spinal Cord in Newborns. Radiographics, n.d. Web. 09 Feb. 2017.
https://www.researchgate.net/publication/221981217_Regional_anesthesia_in_children_The_future
Click to access neonatalspine.pdf
http://pubs.rsna.org/doi/full/10.1148/radiographics.20.4.g00jl06923

Hi I was taught to count coccyx then s4 and back but from your pics I’m doing it wrong if an ossified coccyx is present. Does this depend on age?
LikeLike
Yes sometimes the coccyx is not ossified but with a 15mhz transducer you can still see it the cartilage. I count from the coccyx I find the lumbosacral junction and count from there and I also count from the last rib which is t12 just to be sure
LikeLike