

Introduction
Multiple Sclerosis is a chronic progressive neurodegenerative disorder that can affect the brain, spinal cord and optic nerve. It does so via immune mediated damage to the myelin sheath, a modified plasma membrane that surrounds the nerve axon [1]. It is an autoimmune inflammatory disease that causes demyelination which in turn leads to the development of lesions or plaques. Pathological examination of the lesions shows myelin loss, oligodendrocyte destruction and reactive astrogliosis [2]. Myelin is located in both the peripheral and central nervous systems, however MS solely affects the central nervous system. The neuronal damage leads to a variety of symptoms including but not limited to: visual disturbances, muscle weakness and sensations such as numbness or tingling “pins and needles”. It is 2 to 3 more times common in women than men and is usually diagnosed between 20 and 50 years of age. The disease is considered rare and according to a 2010 study it was thought to affect 58 to 95 people per 100,000 in the United States which translates to approximately 400,000 people [3]. A new study published in the Journal Neurology and supported by the National Multiple Sclerosis Society estimates that in 2017, nearly 1 million adults (up to 913,925) were living with MS in the United States [4]. Given that there are so many suffering from this disease, increased awareness can lead to further research into treatments. Increased awareness has led to MS Awareness and Education Month which lands on March, World MS day and MS awareness week which happen in May. The cause of MS is mostly unknown, though there are factors that have been hypothesized that can trigger the disease like exposure to chemicals and infectious diseases in conjunction with a supposed genetic predisposition. However some of these hypothesis remain unproven.
Signs and Symptoms
Symptoms of MS are typically neurological and episodic in nature. Symptoms can affect different parts of the body and can occur months or years apart. There is no set of symptoms that are pathognomic for MS. MS also shares these symptoms with many other disorders. The diagnosis of MS is a clinical decision made with patient symptoms and laboratory and imaging findings.
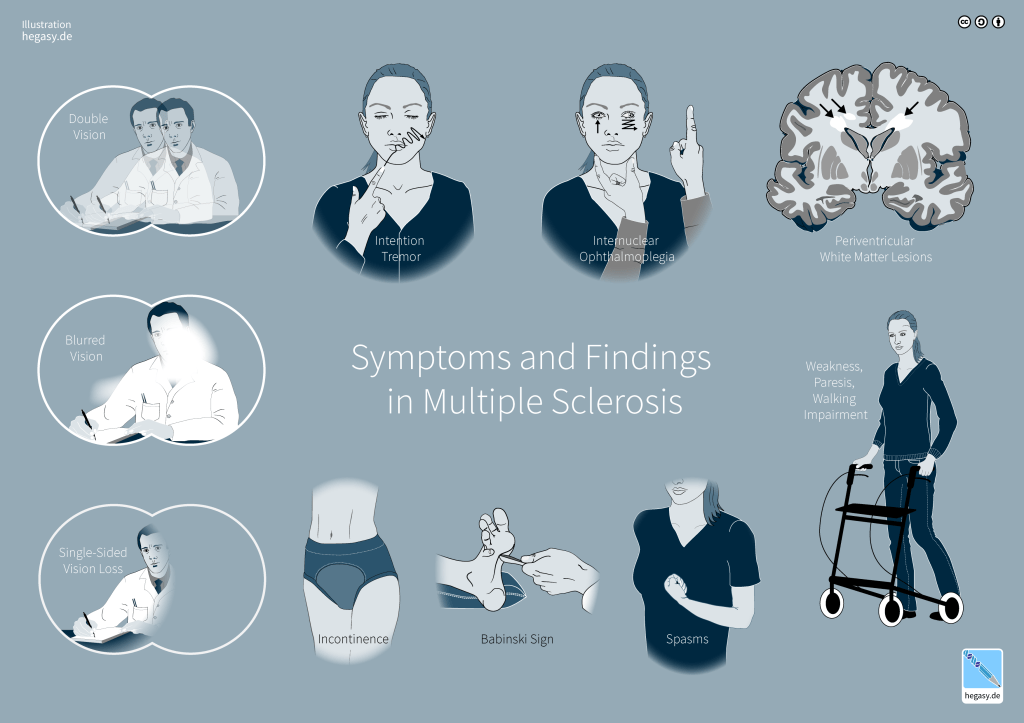
Here is a list of symptoms
- Paresthesia (burning, numbness, pricking or tingling in the arms, legs, feet or anywhere on the skin)
- Muscle cramping secondary to spasticity
- Fatigue
- Charcot triad of dysarthria: broken up speech, nystagmus, and intention tremor
- Optic neuritis (Inflammation of the optic nerve)
- Trigeminal neuralgia: Shooting a jabbing pain, like an electric shock from damage to the trigeminal nerve
- Facial myokymia (irregular twitching of the facial muscles)
- Heat intolerance
- Pain
- Urinary Incontinence
- Bowel problems (constipation, fecal incontinence)
- Issues with attention span, concentration, memory, and judgment
- Clinical Depression
- Bipolar disorder
- Dementia (rare, presents later)
Classification
There are 3 types of MS
Relapsing Remitting (85% of cases)
Secondary Progressive
Primary Progressive
Relapsing Remitting MS (RRMS)
Is the most common type affecting at least 85 5 of patients with MS. [5] It presents as new onset of symptoms followed by a time of being symptom free. The new symptoms may linger on longer and longer as the diseases progresses. These symptoms are described as flare ups or relapses. RRMS is usually diagnosed earlier than its progressive counterparts. RRMS is usually diagnosed earlier in patients 20-30’s, though not as common, some cases have been diagnosed in the pediatric population.
Secondary progressive MS (SPMS)
SPMS begins initially like RRMS. There could be times where the disease is active or not active but with progression of neurological deficits or accumulation of disability over time. Some with RRMS eventually progress to SPMS. Patients with SPMS report more incidence of disabilities that require assistance like using a cane or wheelchair.
Primary Progressive MS (PPMS)
Is characterized by gradual and increasing neurologic deficits from the inception of symptoms, without evidence of relapses or remissions. The disease can be marked with periods of being active (evidence of new lesions on MRI) or not active. It is the more severe form of the disease. People with PPMS tend to develop fewer lesions or plaques, but their lesions seem to be more focused on the spine. Approximately 15 percent of people with MS are diagnosed with PPMS.
Diagnostics
Multiple Sclerosis is diagnosed by a combination of clinical, laboratory and imaging findings. Historically MS could not be diagnosed after a single attack though new criteria has been developed to improve diagnosis even after a single attack. Giving the fact that other diseases have similar symptoms it can prove difficult for clinicians to diagnose the condition. There is often a delay in diagnosis due to many factors, i.e. patients attributing their symptoms to stress or injury, or physicians attributing their symptoms to other causes including psychogenic ones or the symptoms being so mild they may not worry the physician enough to order appropriate test. [5]
Another thing to keep in mind is everyone’s experience of MS is different, the heterogeneity of the disease being attributable to the location of lesions in the nervous system.
There is not one test that can diagnose MS, no magic bullet. Instead the disease is identified by a collection of tests, clinical symptomatology and a set of guidelines called the McDonald Criteria.
The tests that are routinely used in the diagnosis of MS are MRI, Lumbar puncture and Evoked Potential Test.
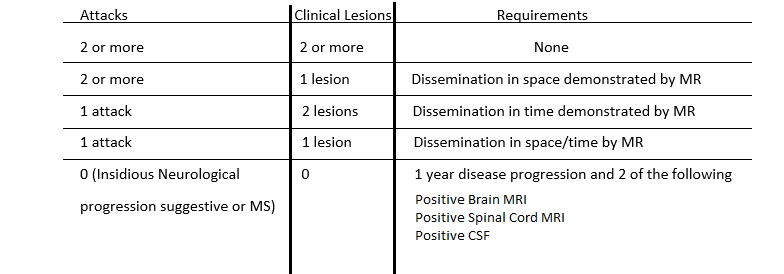
McDonald criteria
McDonald criteria is a diagnostic system used to diagnose MS. It relies on evidence of CNS damage disseminated in time and space, time representing damage occurring in different anatomical locations and time representing lesions occurring at different times in the presence of no better pathological alternative. It had been revised several times the last one being in 2017.
Here is a diagram representing the criteria
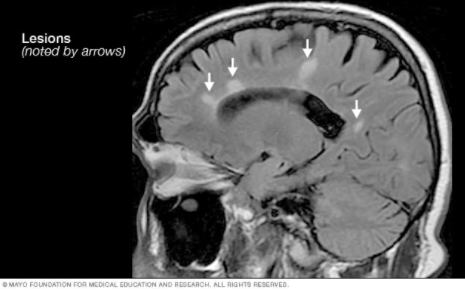
MRI
MRI is a diagnostic radiological exam. It is often used in the diagnosis of MS. The exam can be down with or without contrast. Contrast is an Intravenous agent used to highlight the lesions or area of interest. The contrast typically used in MR is gadolinium.
Findings consistent with MS are usually high signal white matter lesions in the brain and spinal cord.
Cerebrospinal Fluid (Lumbar puncture)
Findings consistent with MS are immunoglobulins (proteins) called oligoclonal bands within the CSF. Also an elevated immunoglobulin (IgG) index provides evidence for intrathecal production of immunoglobulins.
Evoked Potential Test
Evoked potential test is a diagnostic tool to measure the time it takes the brain to respond to a stimulus. An abnormal exam results in a delay or absence in sensory evoked potentials. [7]
Treatment
MS treatments are divided into 3 categories: Treatment for acute attacks, disease modifying treatment and symptomatic therapy.
Acute Attacks
If the patient is experiences a true acute episode or relapse as opposed to a “pseudoexacerbation”, the preferred treatment is glucocorticoids. They provide short term relief by reducing inflammation and duration of attack. The drug of choice is methylprednisolone given as an intravenous medication, sometimes followed by a course of oral prednisolone gradually. This treatment does however have side effects including fluid retention, weight gain, potassium loss and emotional lability. [6]
Disease Modifying Therapies
There are several agents approved by the FDA for treatment of MS relapse. These drugs belong to a class called Interferons, a group of proteins released by cells in response to viruses. Mitoxantrone, which is an immune suppressant, has also been approved for us in the US, though used as a last resort for treatment resistant patients due to its toxicity. A great amount of patients receive IFN-β (Avonex) as a first line therapy. Depending on the frequency of attacks the treatment can be changed (i.e Avonex is not stopping the flare ups). There is not robust evidence on the long term efficacy of this treatment, though recent studies are favorable.
Symptomatic Therapy
Patients with MS may have a host of symptoms that may not respond to therapies aimed at treating the myelin sheath damage. These symptoms may range from pain to psychiatric. Many things should and can be considered to resolve MS associated symptoms. Many patients with MS seem to have low levels of vitamin D, in fact MS is more common the further you get away from the equator due to lack of sunlight suggesting a link between sun exposure, vitamin D and MS. Recent studies have shown a positive influence on vitamin D supplementation on MS symptoms, further research is needed to determine whether there is a causal effect of hypovitaminosis D and multiple sclerosis.
Furthermore many physicians and lay persons alike recommend certain diets and exercise (whatever type that is tolerated by the patient given their disability burden). Many patients also benefit from Physical Therapy and Counseling or Psychological therapy. Depending on the severity of their emotional or psychological issues, psychiatric consultation is recommended with possible psychopharmacotherpay.
Multiple Sclerosis is a complex, progressive neurological disorder that requires the specialty treatment of neurologists and a multidisciplinary team of healthcare workers the disease affects its sufferers differently. There is no cure for the disease, however there is increasing awareness and research that one day may lead to more effective treatments.
Bibliography
- Morell, Pierre. “The Myelin Sheath.” Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th Edition., U.S. National Library of Medicine, 1 Jan. 1999, www.ncbi.nlm.nih.gov/books/NBK27954/.
- Multiple Sclerosis. (2019, February 22). Retrieved from https://emedicine.medscape.com/article/1146199-overview#a3
- Noonan CW, Williamson DM, Henry JP, et al. The prevalence of multiple sclerosis in 3 US communities. Prev Chronic Dis. 2009;7(1):A12.
- Lorene M. Nelson, Mitchell T. Wallin, Ruth Ann Marrie, W.J. Culpepper, Annette Langer-Gould, Jon Campbell, Stephen Buka, Helen Tremlett, Gary Cutter, Wendy Kaye, Laurie Wagner, Nicholas G. Larocca, for the United States Multiple Sclerosis Prevalence Workgroup
Neurology Mar 2019, 92 (10) 469-480; DOI: 10.1212/WNL.0000000000007044
- Cecil, R. L. 1., Goldman, L., MD., & Schafer, A. I. (2012). Goldman’s Cecil medicine (24th ed.). Philadelphia: Elsevier/Saunders
- Kasper, D. L., Fauci, A. S., Hauser, S. L., Longo, D. L. 1., Jameson, J. L., & Loscalzo, J. (2015). Harrison’s principles of internal medicine (19th edition.). New York: McGraw Hill Education.
