

Authors: Henry Suarez RDMS, RVT; Richard Garay R.T. (S), RDMS, RVT
Hemodialysis
Hemodialysis is a medical procedure that uses a dialysis machine to filter wastes and water from your blood in cases of renal failure. In order to use a hemodialysis machine the patient needs access to their blood supply. This is achieved with a hemodialysis vascular access device.

There are 4 types of vascular access devices.
- Central venous catheter
- Arteriovenous fistula (AV Fistula)
- Arteriovenous graft (AV Graft)
- Peritoneal dialysis catheter
We’ll be discussing two in this article; AV Fistulas and AV grafts.
Arteriovenous Fistula
Arteriovenous Fistulas or AV-Fistulas/AVF is created by surgically anastomsing a native artery and vein together, usually the radial artery to cephalic vein commonly known as Brescia-Cimino fistula. The non dominant arm is typically used for fistulas. Prior to the surgical procedure the patient will undergo vein mapping to establish whether their vascular anatomy is amenable for fistula.
Locations
- Radial artery to cephalic vein (Brescia-Cimino)
- Ulnar artery to basilic vein

The benefits of Arteriovenous Fistula (AVF) is that it has the lowest rate of failure and complications as you are using the patients native tissue. Fistulas created with small-caliber veins (<1.6 mm) are at high risk for early failure
Once the AV fistula creation is complete, you will need to wait several months for it to fully heal and mature before use.
Arteriovenous Graft
An AV-graft is also created surgically by using a small hollow, synthetic tube that connects the artery to the vein. The material used is usually a Polytetrafluoroethylene (PTFE) aka Gore-Tex tube. Grafts are used as opposed to fistulas when the patient’s native vasculature is not suitable for fistula creation. The graft can be straight or looped.
Locations
Straight
- Distal radial artery to cephalic, median cubital or or basilic vein
- Distal brachial artery to proximal basilic vein
Loop
- Distal radial artery to cephalic, median cubital or or basilic vein
- Proximal brachial artery to axillary vein
- Femoral artery to great saphenous vein

Waveforms
Upper Extremity Artery
The normal upper extremity artery has a high resistance waveform and is triphasic.
The flow can become monophasic with high diastolic flow after exercise this is know as reactive hyperemia.
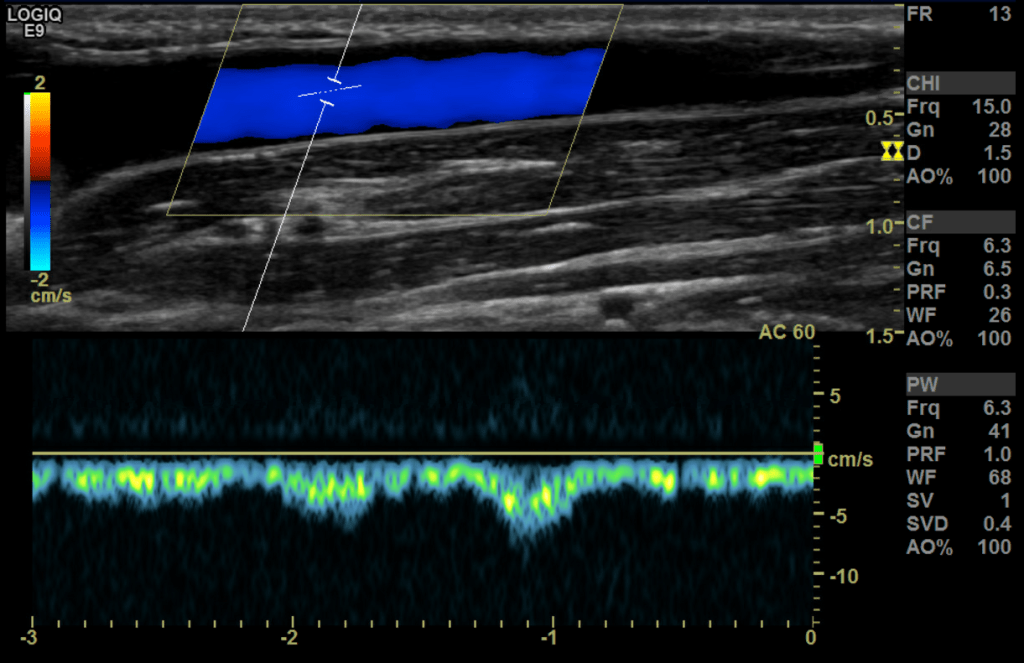
Upper extremity Vein
The flow in a normal vein is monophasic and has very little phasicity with normal breathing and cardiac patterns with increased reversal of flow after distal augmentation
Fistula waveform
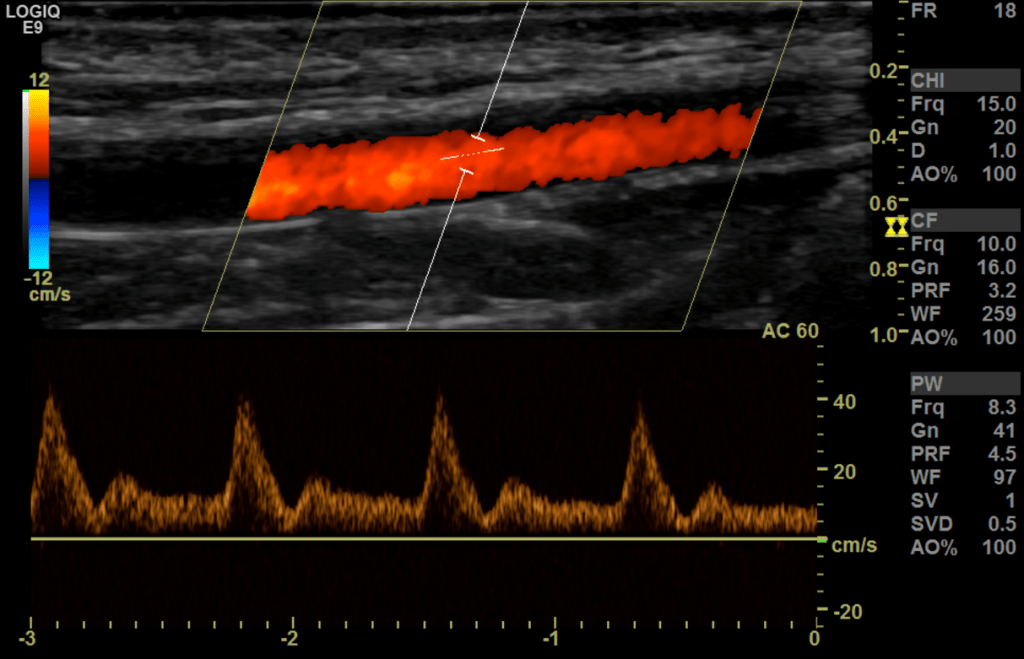
A fistula waveform is going to be high velocity, low resistance in both the artery and the vein. It is often turbulent with spectral broadening. The further away from the anastomosis you go the lower the pulsatility gets.
In normally functioning fistulas, waveforms of flow in the supply arteries and throughout the graft are monophasic, with peak systolic velocities of 100-400 cm/sec and end-diastolic velocities of 60-200 cm/s (stenosis at the anastomosis sight is common and has been determined to not adversely effect graft/fistula function and no association between stenosis and graft occlusion has been found.
sec. The draining veins have arterial pulsations with peak velocities of
30-100 cm/sec.
Protocol
- You’ll want to perform an upper extremity vascular exam. Assessing the vessels from Jugular or Subclavian down to the graft/fistula site.
- Evaluate arterial inflow proximal and distal to the anastomosis.
- Asses the site of anastomosis.
- Scan the proximal, mid and distal sections of the graft/fistula (outflow).
- Pay close attention to previous puncture sites along the graft/fistula.
- Assess for pseudoaneurysm, stenosis, thrombosis, occlusion and collections.
Case Review
This case is to survey an upper extremity hemodialysis AV fistula that we commonly see in the vascular lab.
Use a linear transducer 7-12 MHz .
A patient history of ESRD (end-stage renal disease) is a common indication for most of our frequent hemodialysis patients.
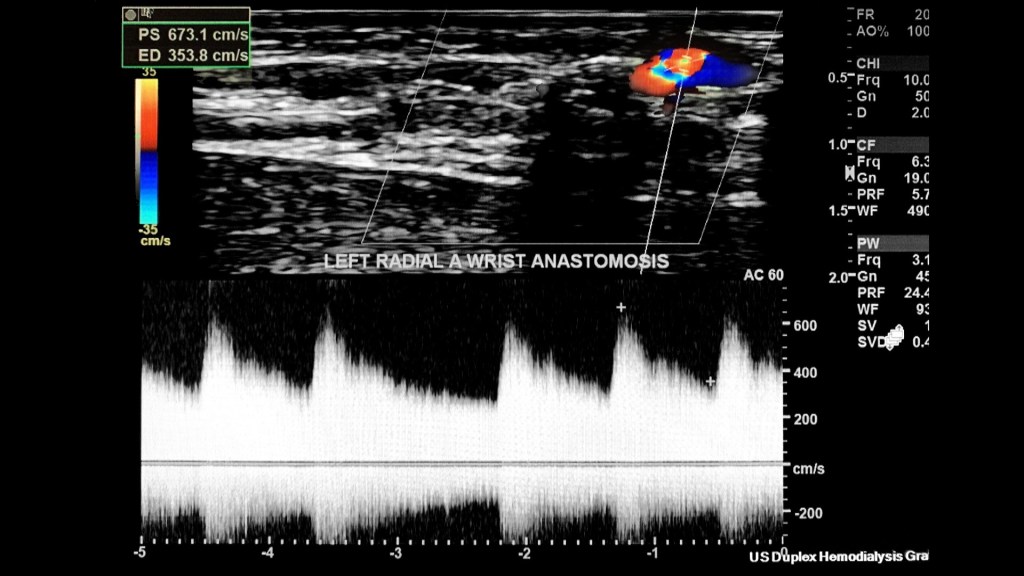
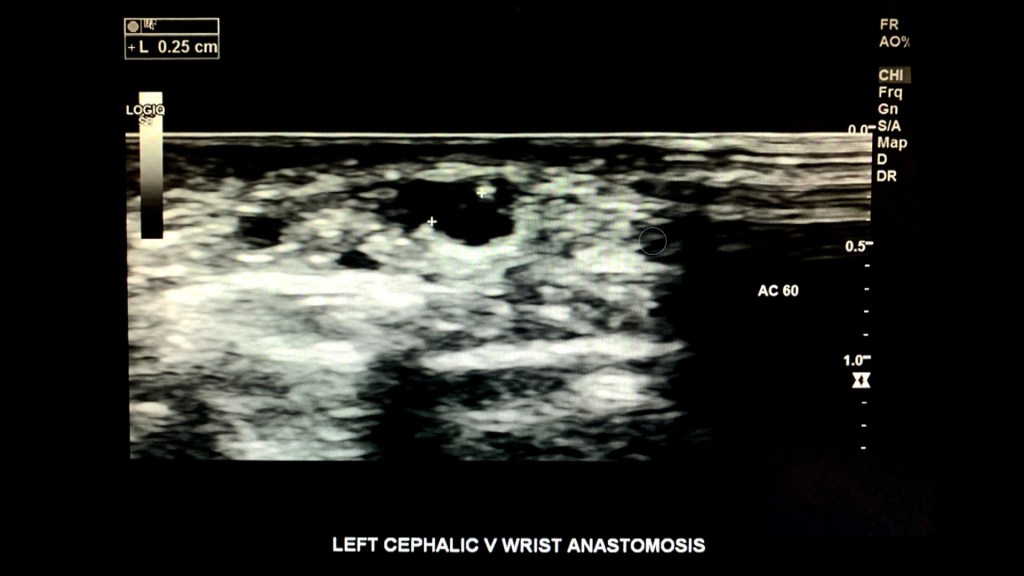
This patient has a left arm radial-cephalic vein AV anastomosis (aka Brescia-Cimino) which is the most common AVF connection.
Evaluate the patency and maturity of the fistula while also monitoring the inflow/outflow streams as well as assessing the site of anastomosis.
In this case the radial artery is the inflow; and the forearm cephalic vein the outflow.
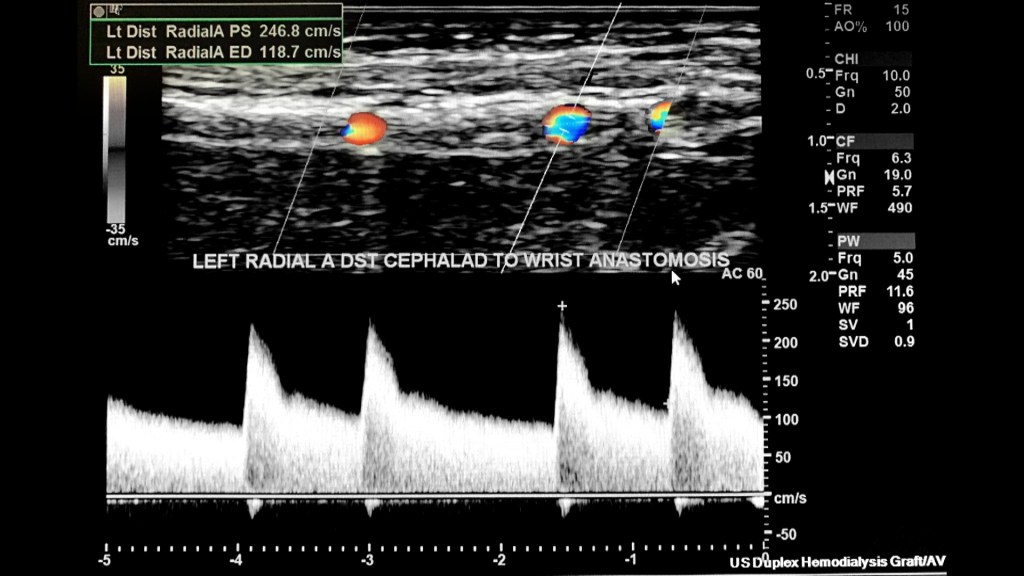
We begin our exam protocol by evaluating the inflow stream proximal to the anastomosis beginning with the subclavian artery followed by the axillary, brachial, ulnar and radial.
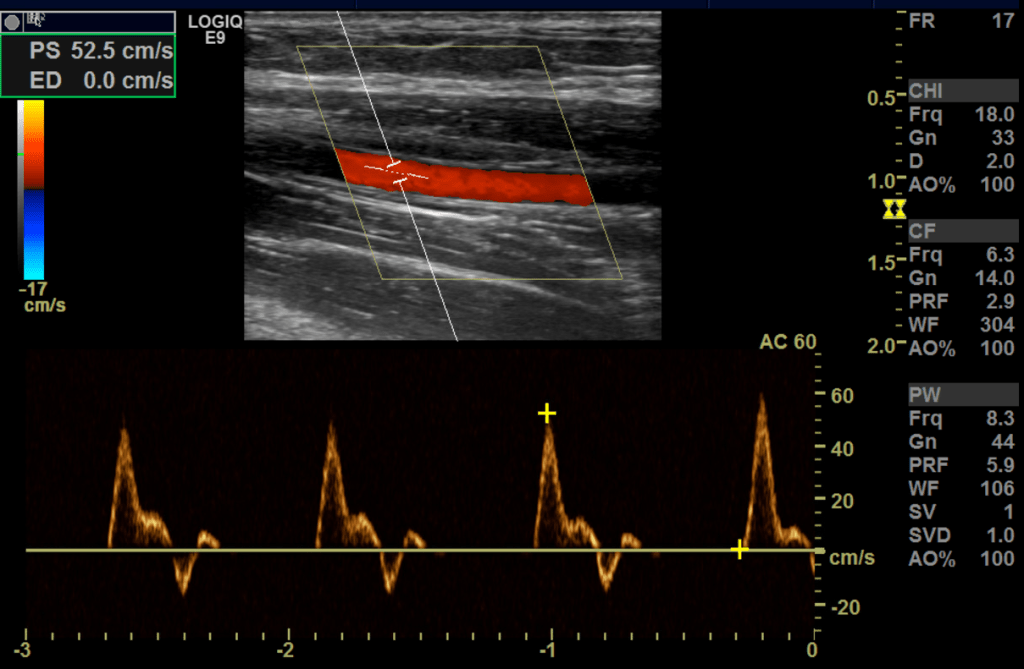
The normal spectral arterial tracing (inflow) proximal to the AVF will be a lower resistant high flow waveform followed by a higher resistance waveform distal to the anastomosis (make sure to evaluate for steal syndrome). The spectral analysis in the radial artery proximal to anastomosis has a high PSV/EDV at 247 cm/s and EDV at 119 cm/s.
I sampled the arterial anastomosis side a few times with the highest PSV/EDV as 673/354 cm/s.
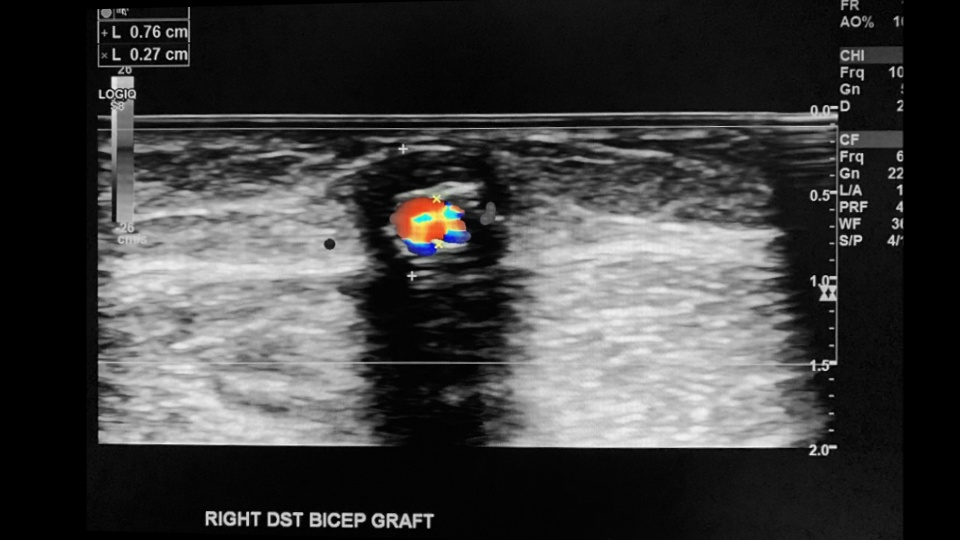
Next we assess the outflow stream (venous side) starting with the subclavian/cephalic vein confluence at the shoulder level followed by the bicep and forearm segments of the outflow stream evaluating for abnormalities such as thrombus, stenosis, occlusions, PSA/aneurysms, etc.

Sample the venous anastomosis side a few times the highest sampled here is PSV/EDV as 500/170 cm/s.
Make sure to measure the size of the anastomosis before completing the exam.

This case proved the fistula was patent and optimally matured.
Complications
As with all medical procedures and surgeries there are complications such as infection and or collection formation (whether abscess or hematoma). The access is also liable to thrombose, suffer from stenosis and pseudoaneurysm.

Thrombosed pseudoaneurysm

Stenosis
Criteria for > 50% stenosis in AV grafts
- Peak systolic (PSV) velocity >400 cm/s
- Velocity ratio >=2:1 (area of stenosis compared/proximal to stenosis)
Criteria for >50% stenosis of AV fistula
- PSV >400 cm/s
- Velocity ratio 2:1 or 3:1
- Velocity measurements may be difficult to acquire or inaccurate in tortuous vessels and variations in vein diameter

Occluded/Thrombosed
Occluded Grafts
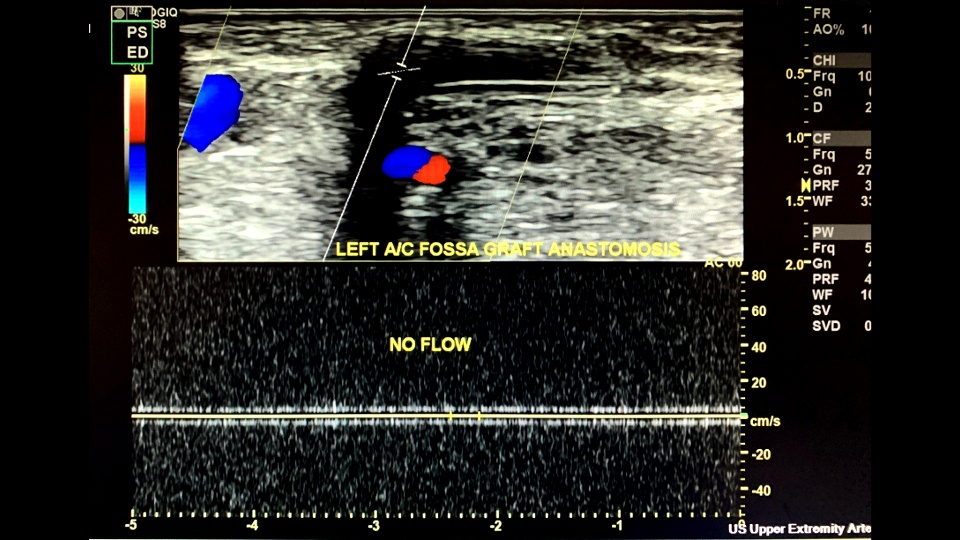
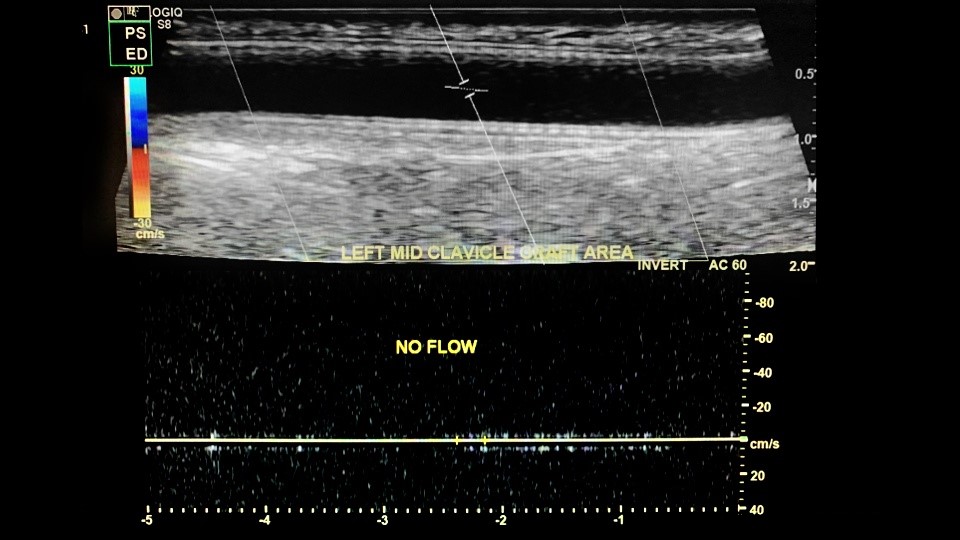
Thrombosed Fistula

Steal syndrome
Steal syndrome is a complication that can occur after the construction of a vascular access for hemodialysis. It results in ischemia of the hand caused by marked reduction or reversal of flow through the arterial segment distal to the arteriovenous fistula (AVF).

Sources:
1.Belli, Sedat, et al. “Surgical Interventions for Late Complications of Arteriovenous Fistulas.” International Surgery, The International College of Surgeons, World Federation of General Surgeons and Surgical Specialists, Inc., 2014, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4114382/.
2. http://www.atcs.jp/pdf/2005_11_1/59.pdf
3. Konner K (2002). “Vascular access in the 21st century”. J. Nephrol. 15 Suppl 6: S28–32.
4. Zamboli, P., Fiorini, F., D’Amelio, A., Fatuzzo, P., & Granata, A. (2014, July 11). Color doppler ultrasound and arteriovenous fistulas for hemodialysis. Retrieved April 13, 2021, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4209216/
