

Transducer
I use a 6 MHz (dropping the frequency between 4-5 if necessary) Curvilinear abdominal transducer and the 9 MHz linear transducer to get higher res doppler, gray scale and bflow images. If the patient is obese you may use a sector transducer.


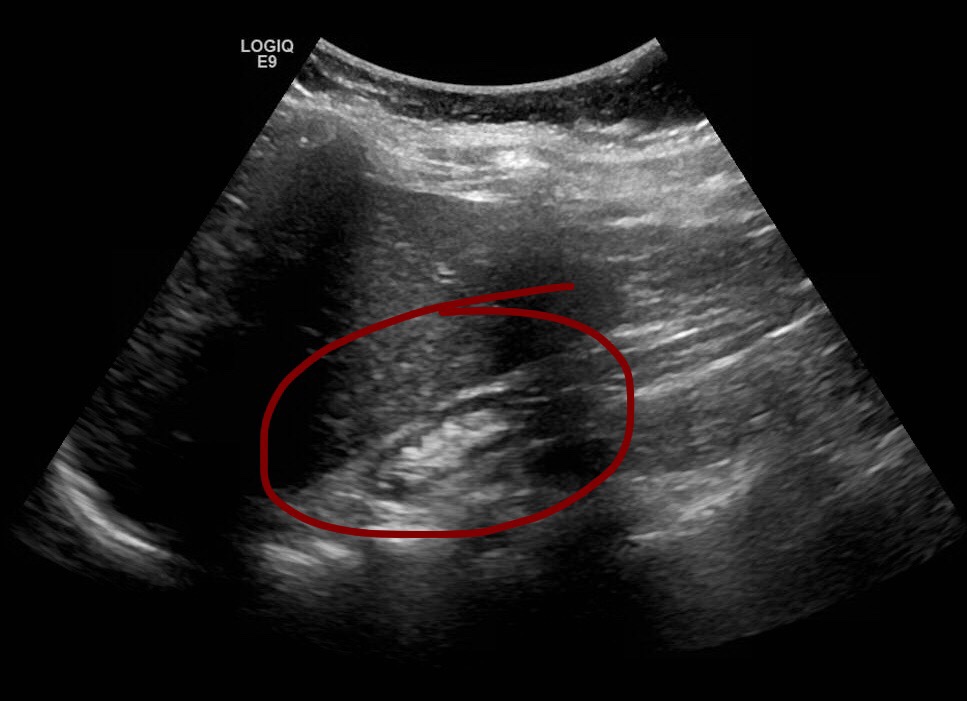
I like to begin the exam examining the native kidneys. Now a transplant recipient is likely to have suffered some chronic kidney disease, as such the native kidneys may be scarred, atrophic and in some cases imperceptible due to sever atrophy or surgery. In either case image the right and left renal fossa.

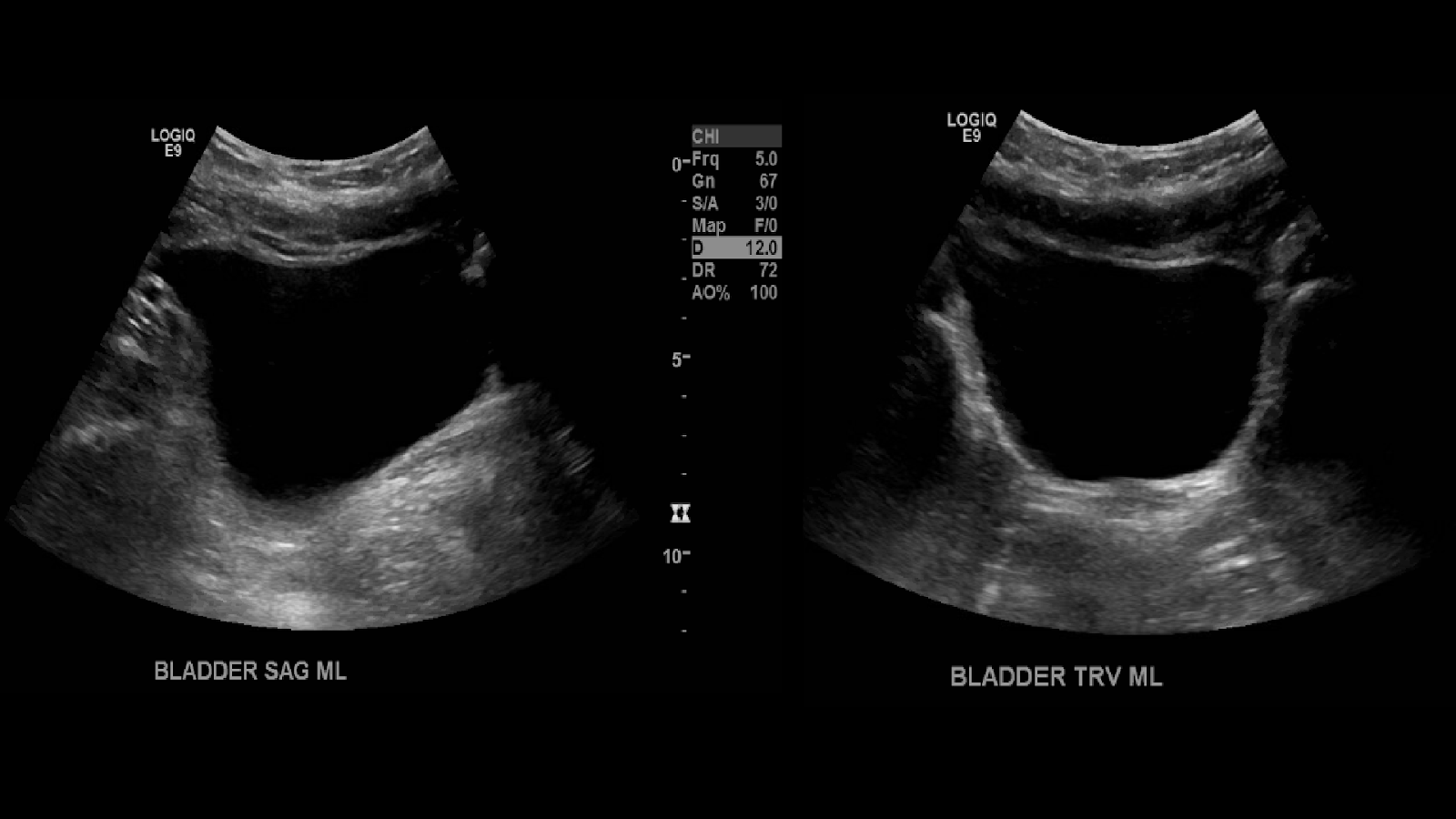
I then move on to image the bladder in sagittal and transverse.
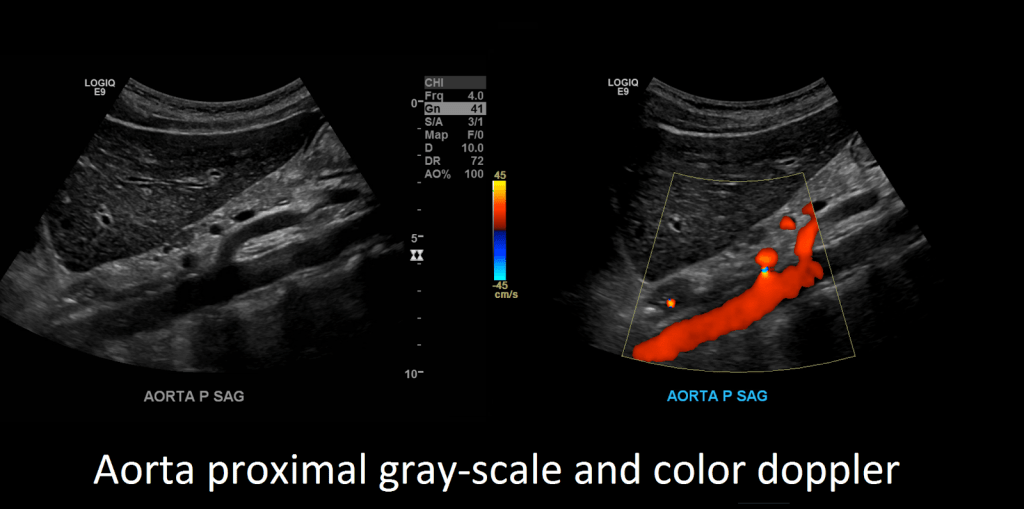
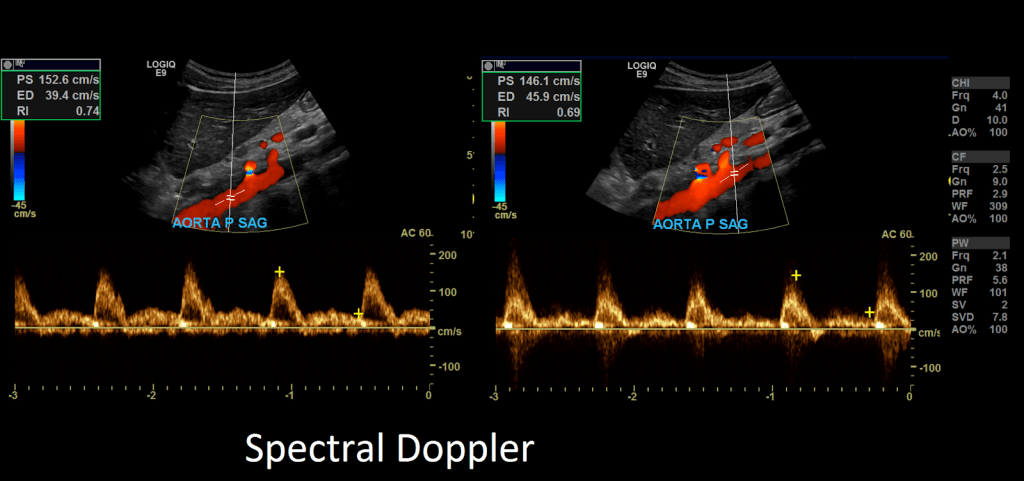
After you’ll want to image the aorta in sagittal and transverse in grayscale and with color and spectral Doppler.

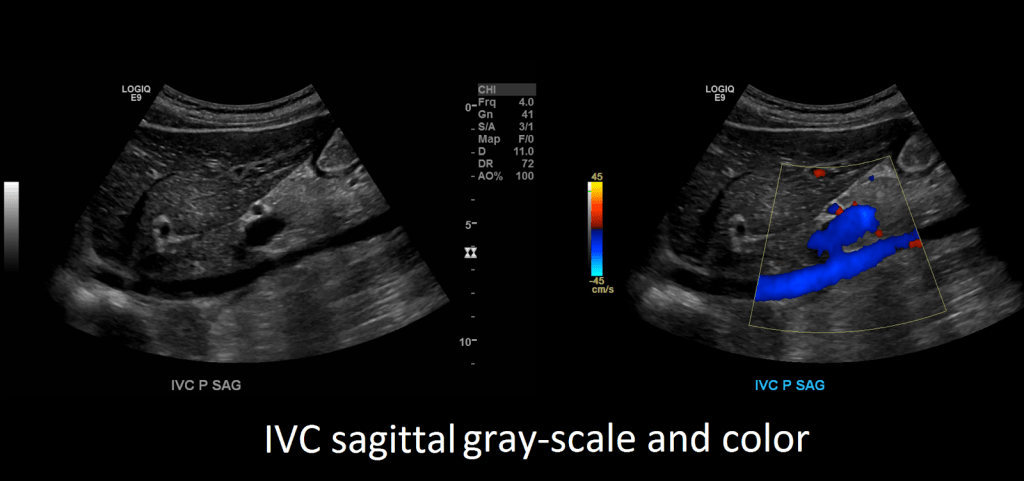
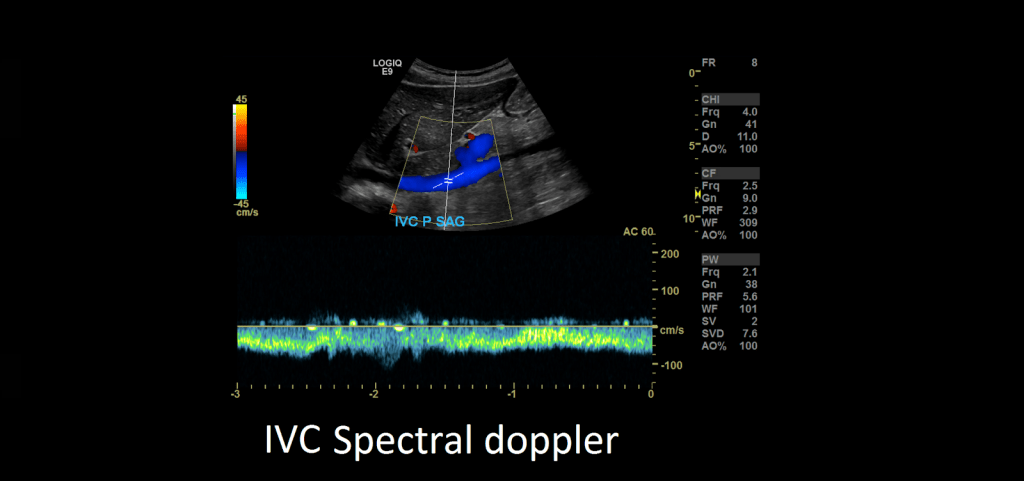
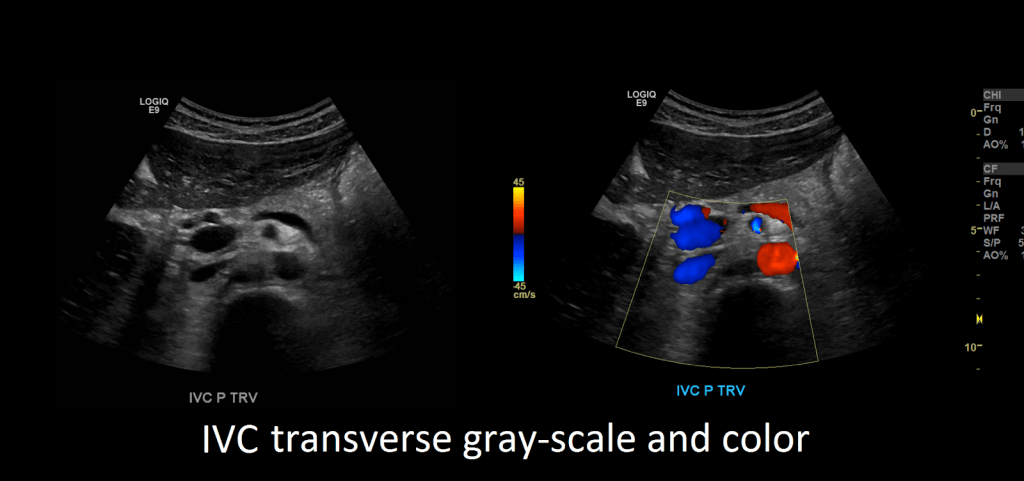
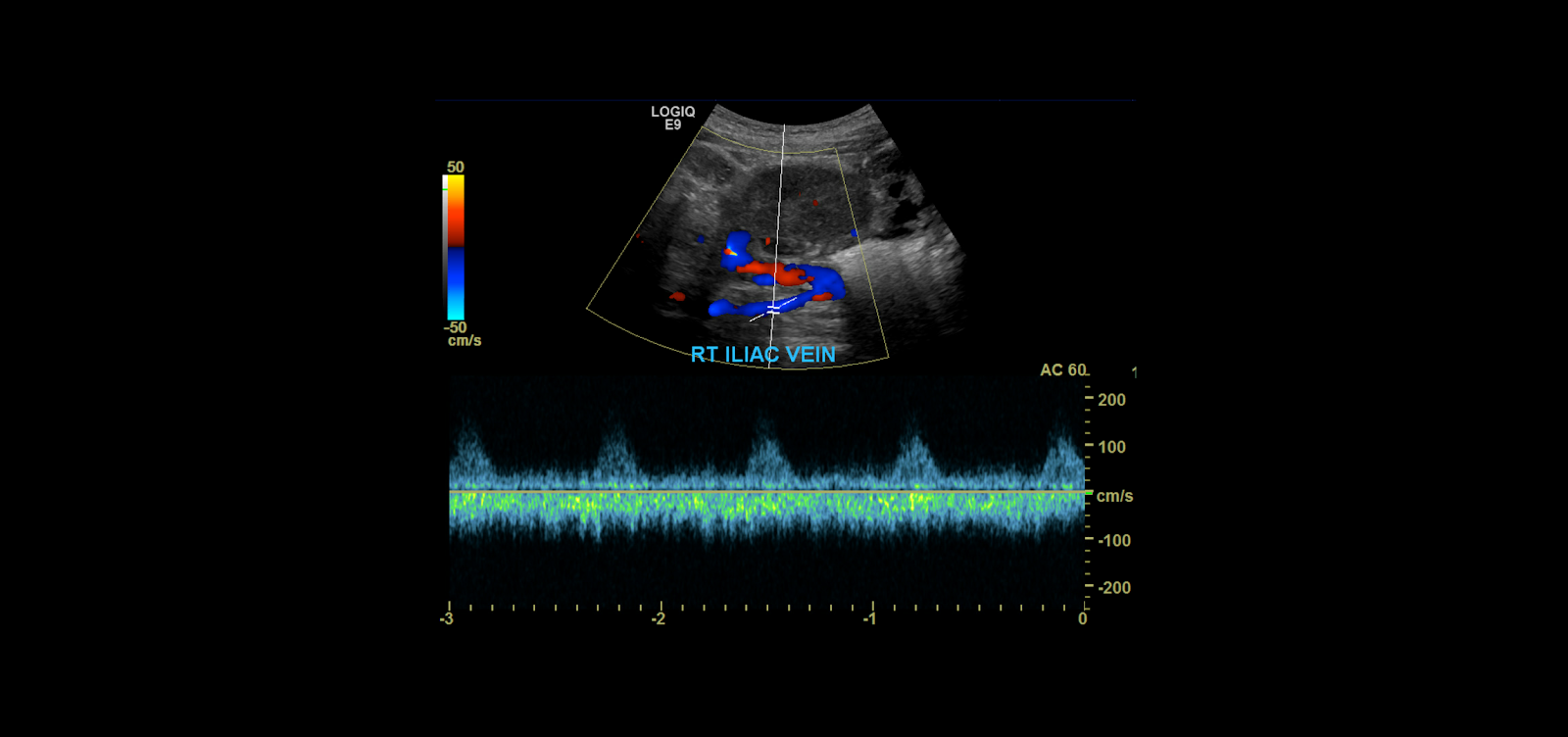
After you’re done evaluating the aorta, turn your attention to the inferior vena cava. Capture images in sagittal and transverse in grayscale, color and spectral Doppler.
Next proceed to evaluate the transplanted kidney. The most common site of implantation is in the right iliac fossa.

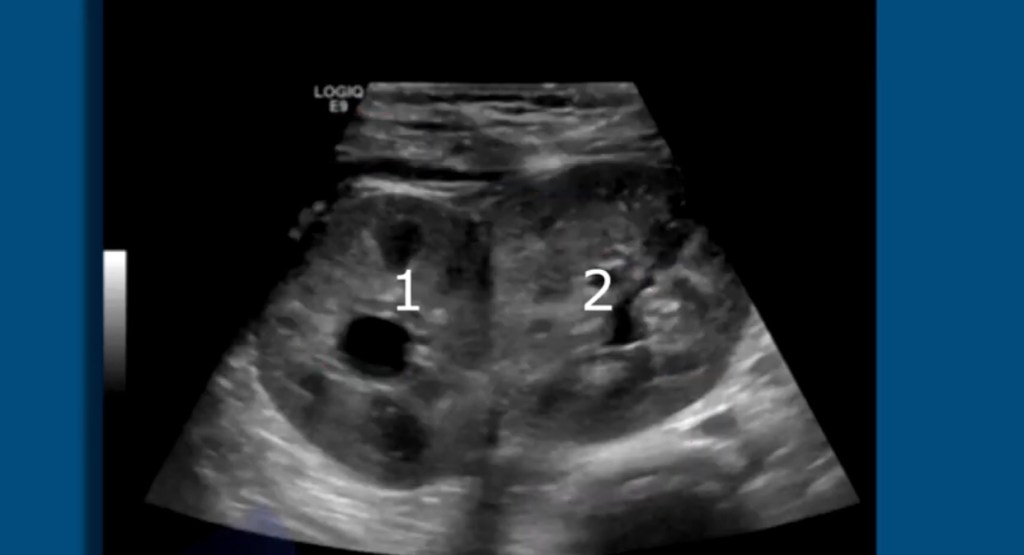
In some cases there may be 2 renal transplants done at once know as en bloc transplant. This is usually done when the donor is less than 5 years of age. Both kidneys get transplanted.
In smaller patients the transplanted kidney will be closer to the liver as their abdomens are smaller.

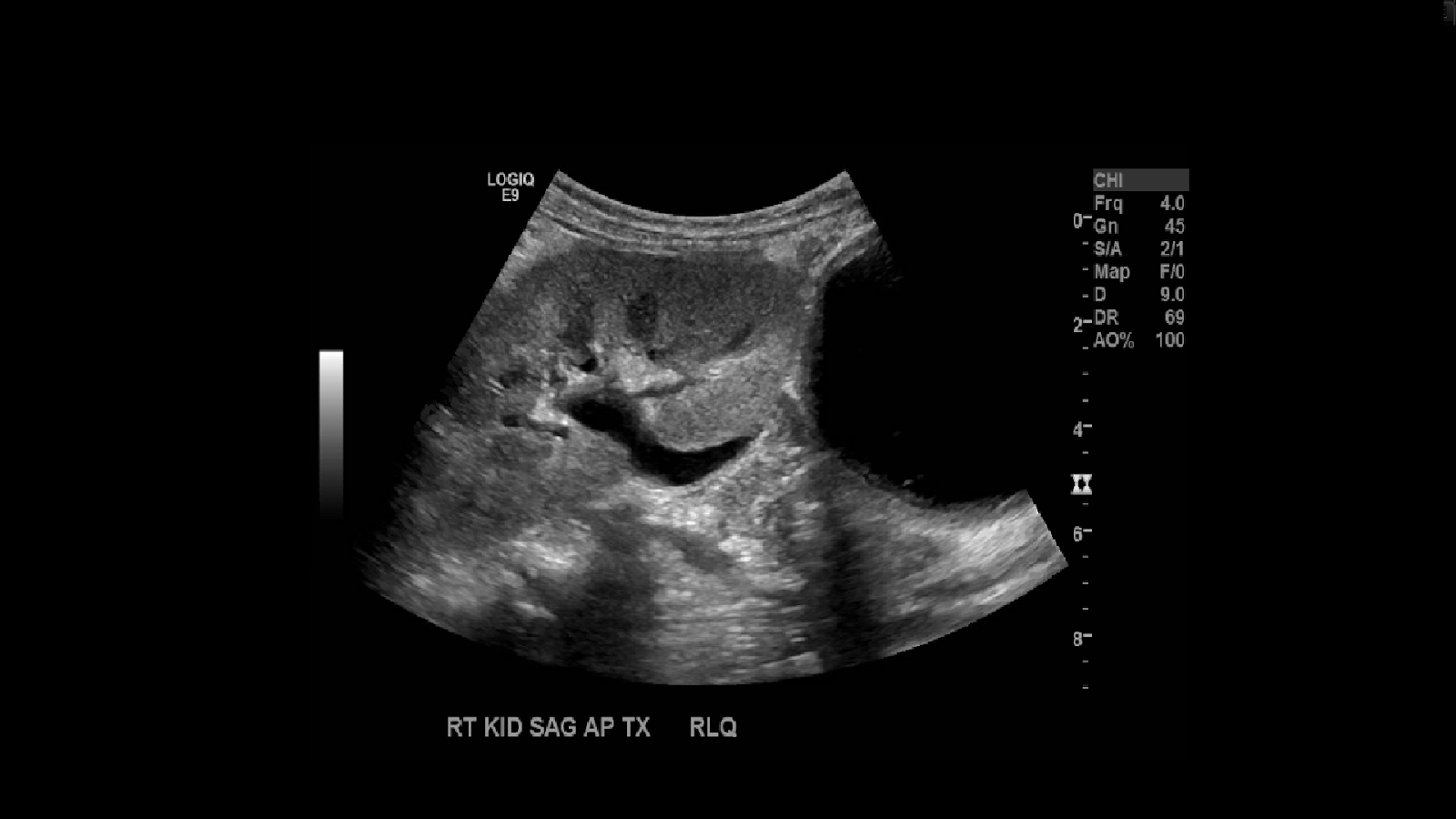
In full sized adults you’ll observe the kidney in the right iliac fossa. Image the kidney in sagittal and transverse planes. Utilize Doppler to see the vascularity. Measure the kidney. If the kidney is too large you can take a panoramic image. Make sure to take not of the echogenicity, check for edema, areas of no vascularity, look for collections.

Doppler
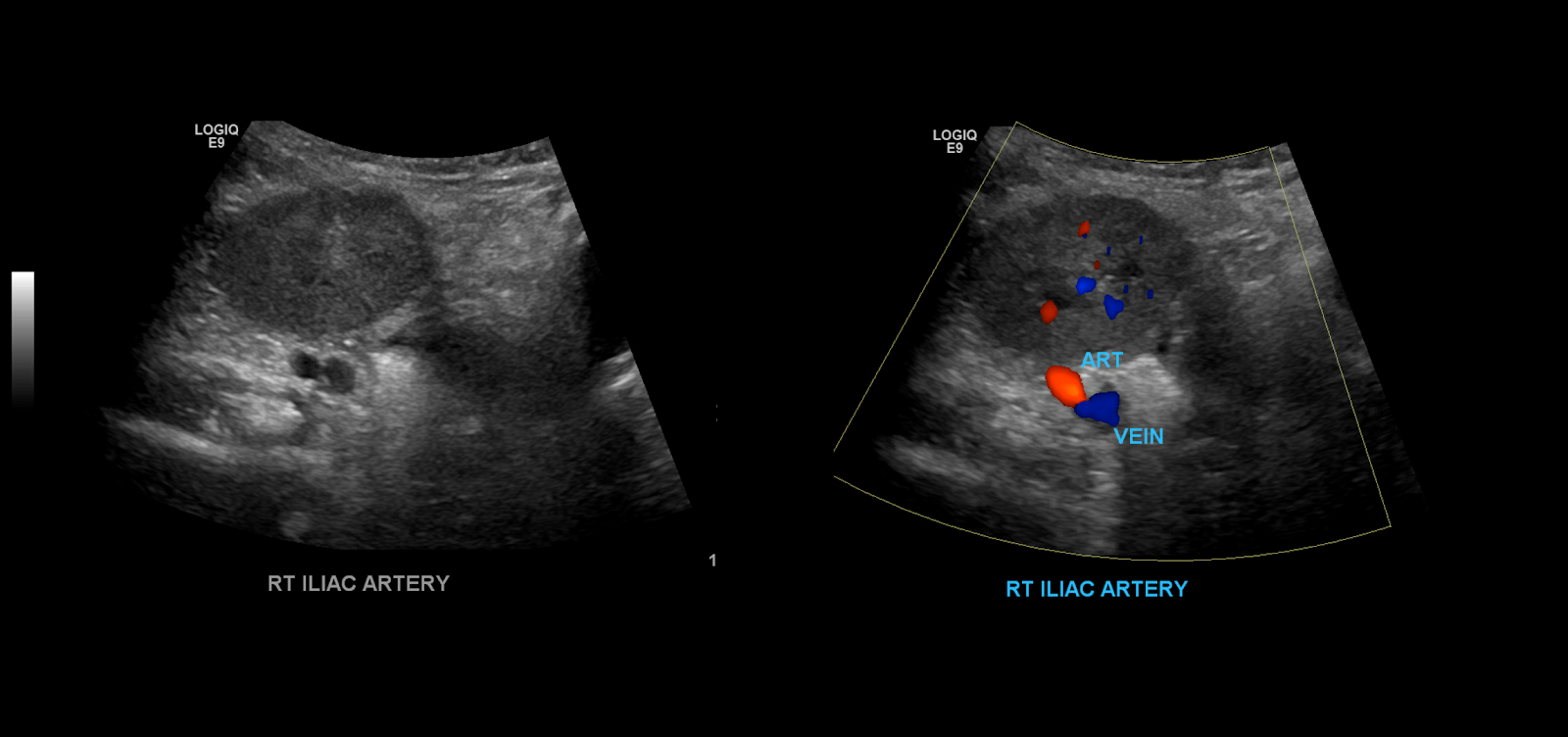
When you’re done examine the kidney in gray-scale you become to take your color spectral Doppler images. Begin with the iliac vessels.
Take gray-scale, color and spectral Doppler of the common iliac artery. Use angle correction 45-60°.
Measure the peak systolic and end diastolic velocities.

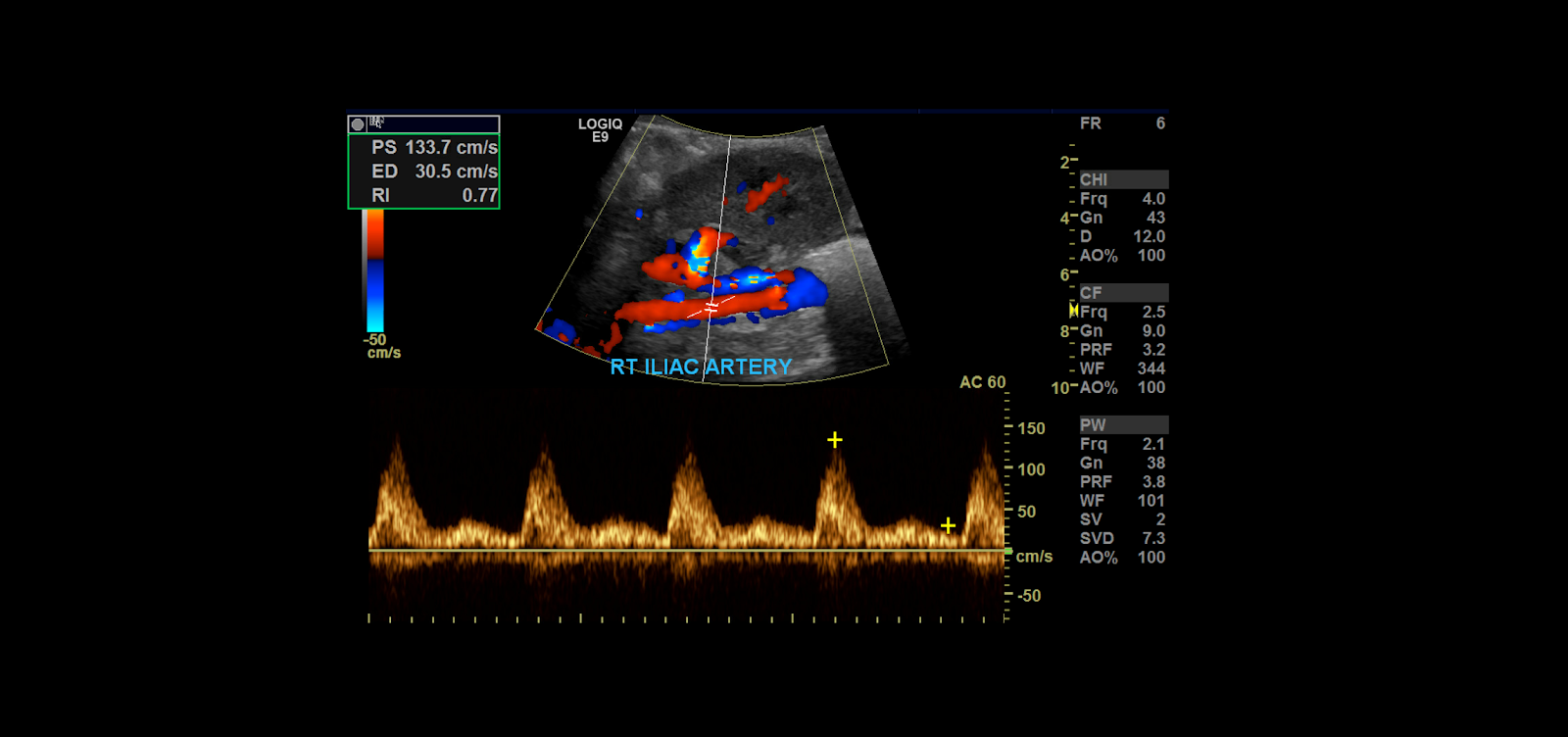
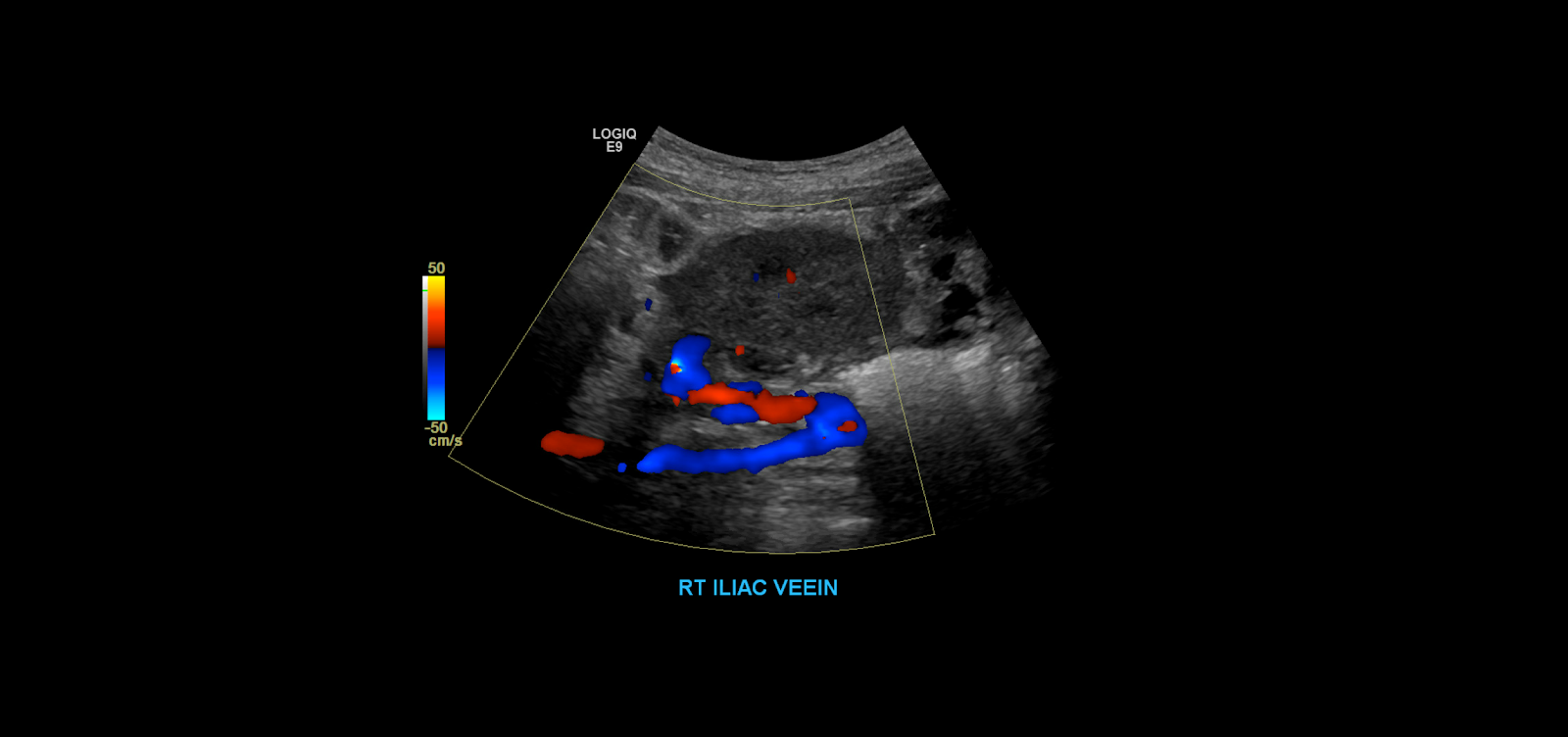
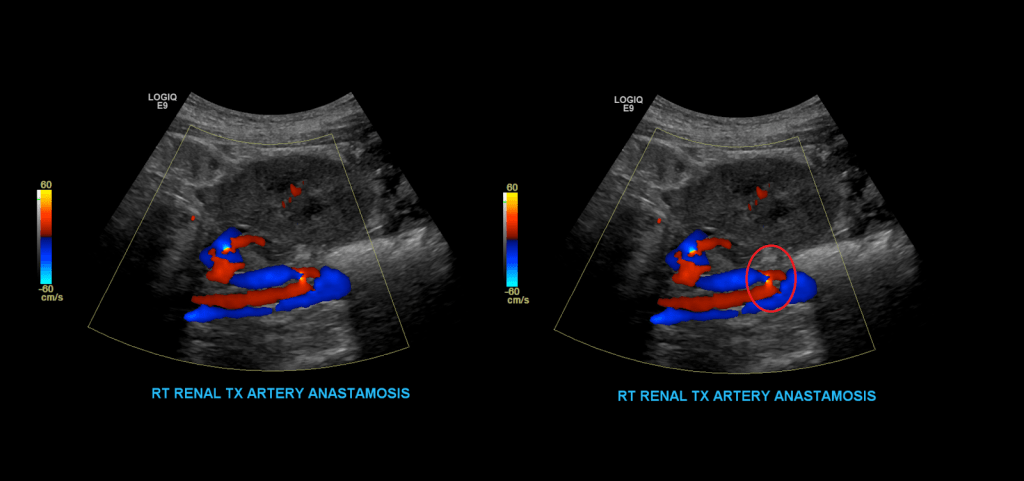
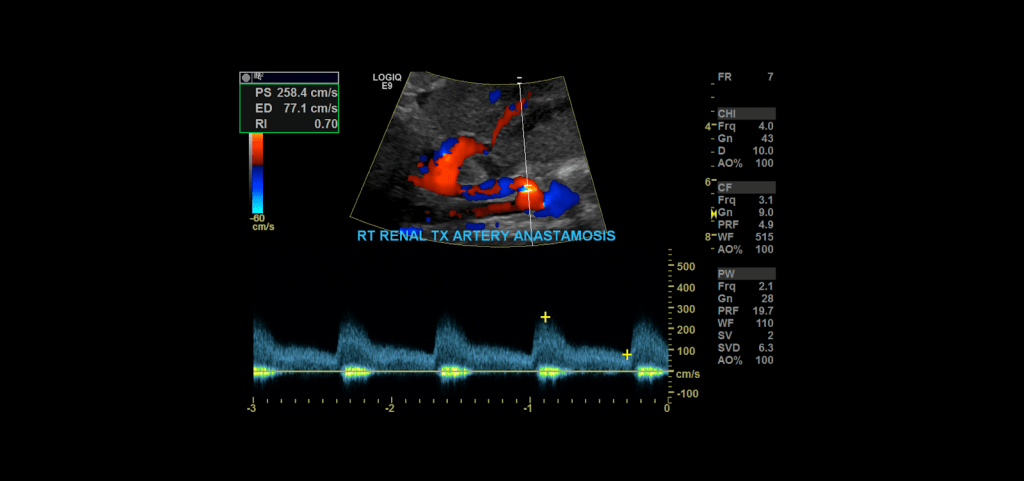
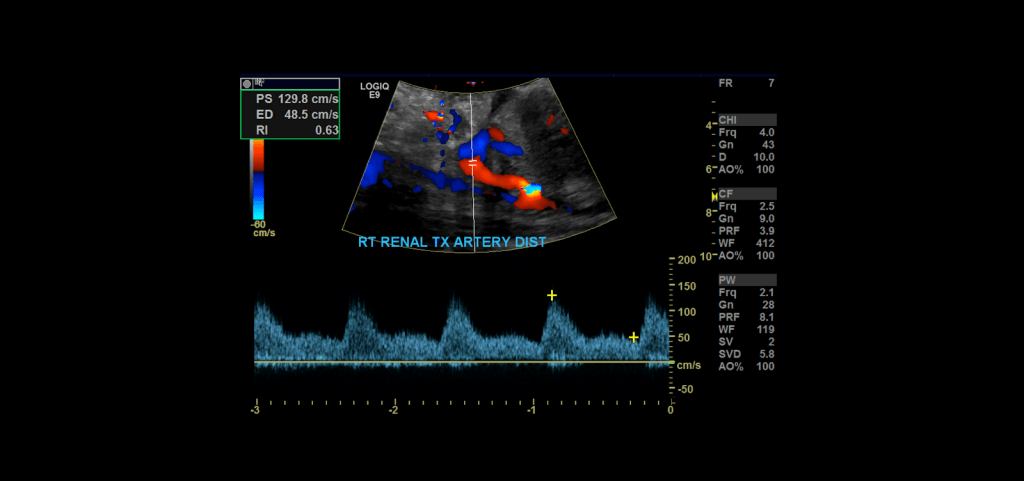
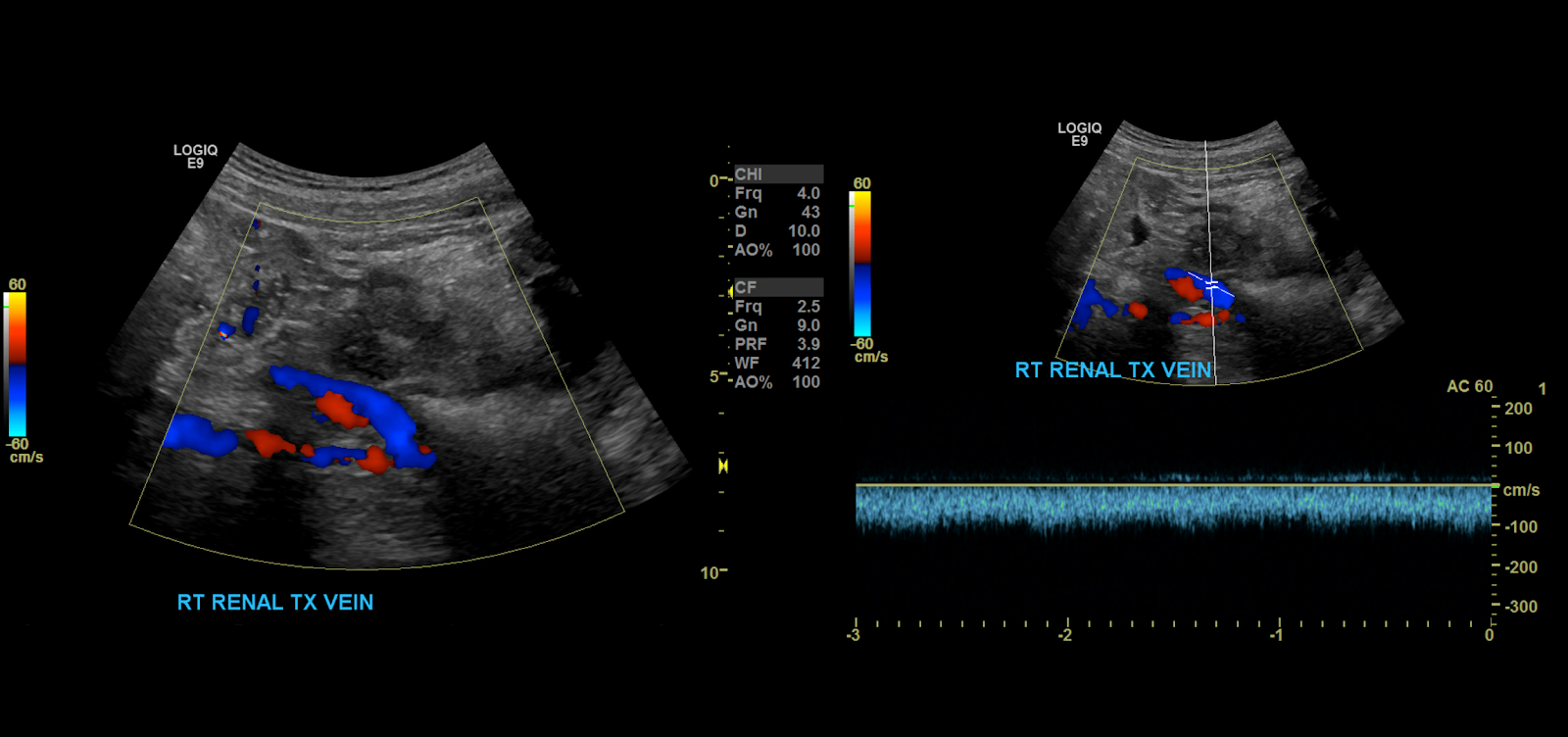
Proceed to doppler the transplant main renal artery and vein. Given the tortuosity sometimes seen in the donor arteries, measuring velocities with angle correction can be tricky. My rule of thumb is that if the artery is perpendicular to the transducer face I don’t use angle correction. If it is parallel to the transducer face I do use angle correction.

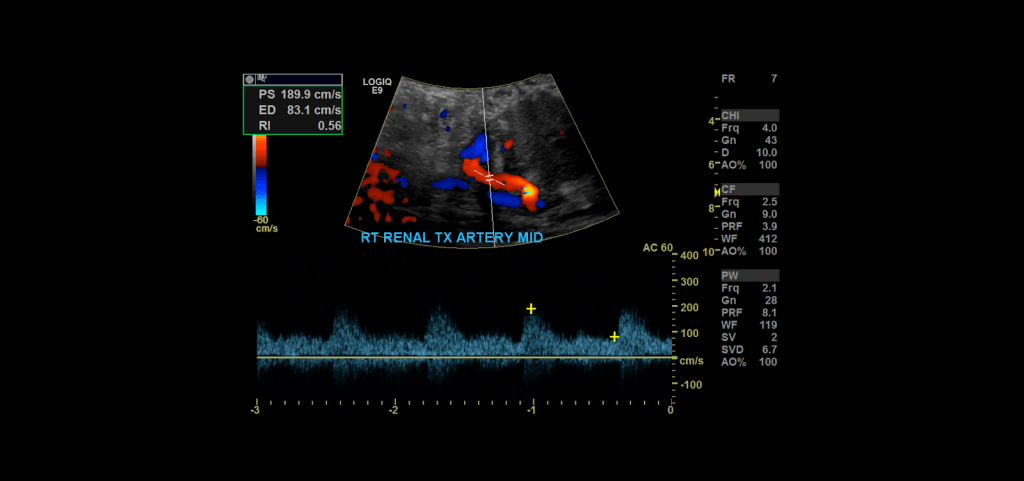
Measure the peak systolic and end diastolic velocity. Resistive Index is normally between 0.50 and 0.70. The waveform should be a low resistance waveform with forward flow throughout the cardiac cycle. Take Doppler samples at the anastomosis/proximal section (pay close attention here look for aliasing to detect anastomotic stenosis), the mid and distal portions as well. If there’s any aliasing along the vessel take spectral Doppler samples there too.
Main Renal Artery
Renal Vein
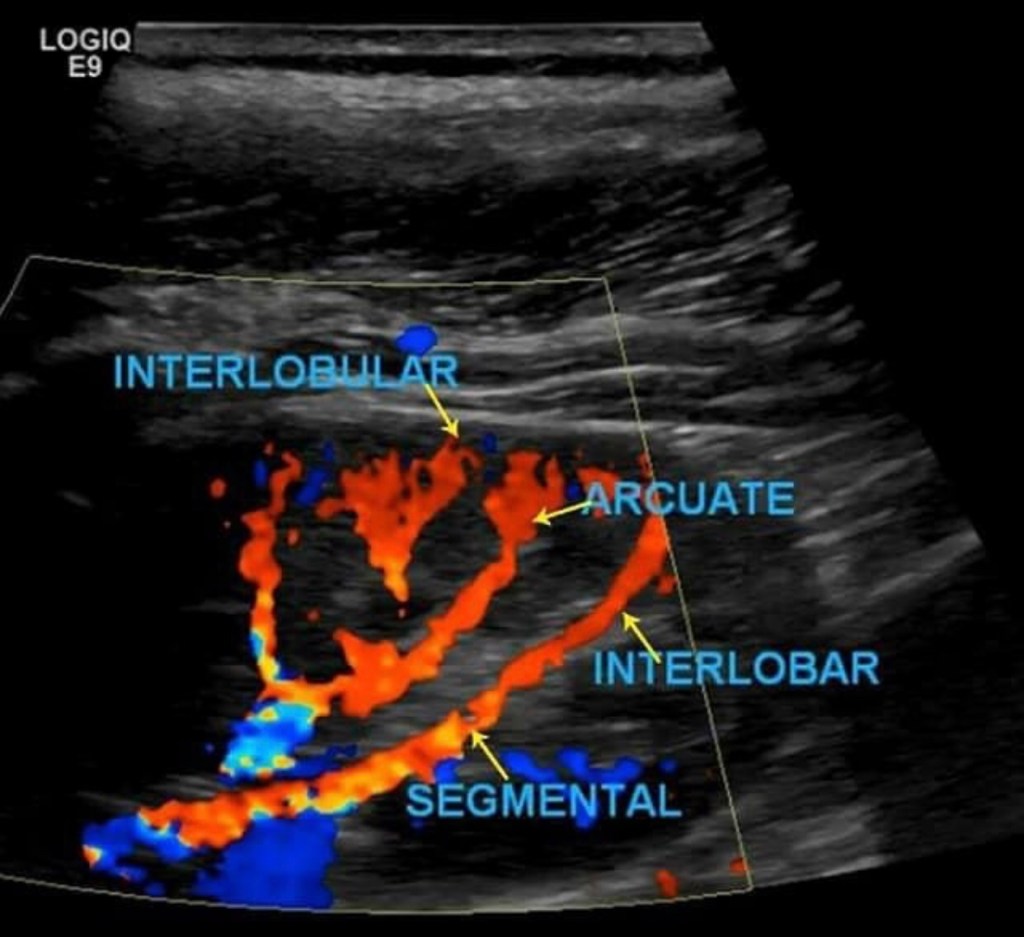
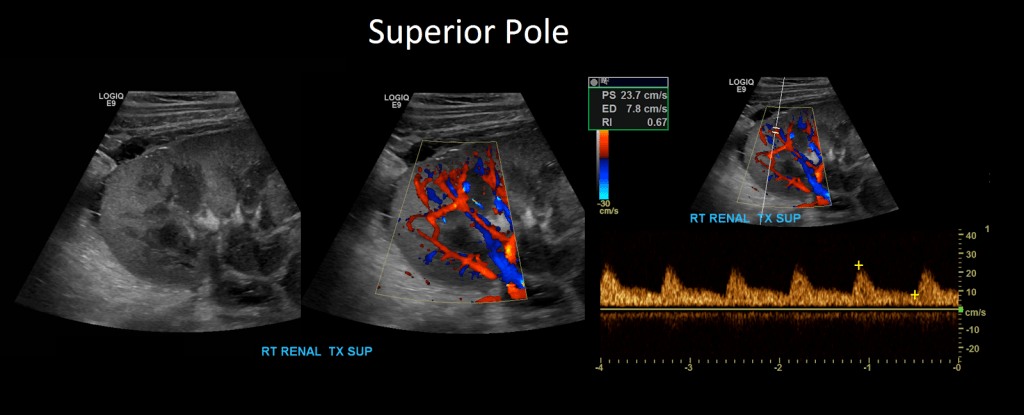
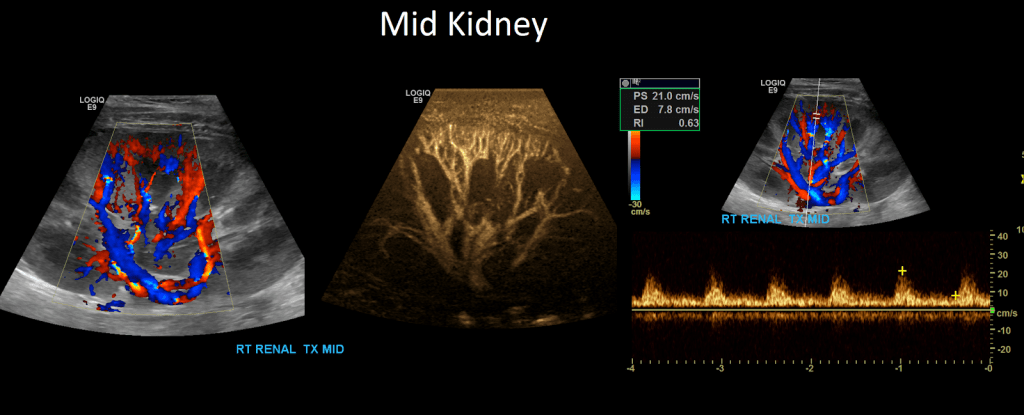
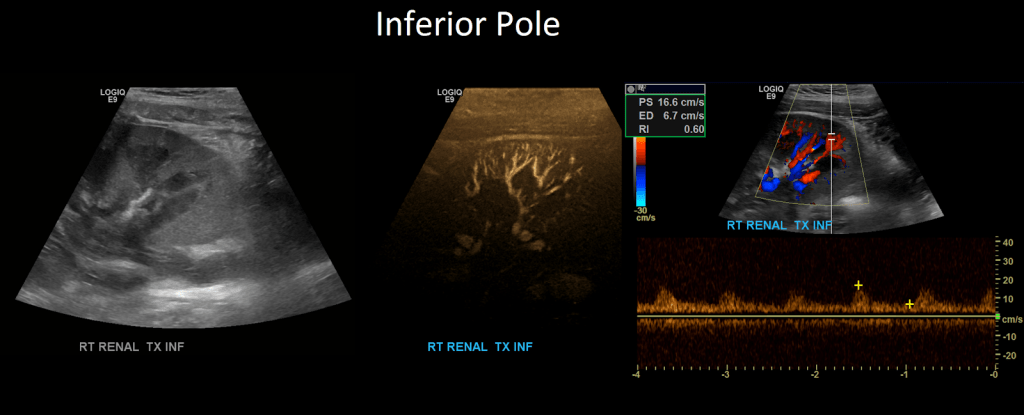
Intrarenal Doppler
Once that is complete move on to Doppler the arcuate/segmental arteries (your institution may require one or the other or both). Doppler these arteries in the superior, mid and inferior pole of the kidney. Do not use angle correction.
And that’s it. If you want some more information watch the video above where I explain it some more. And leave any questions in the comments.

Thank you so much for posting this. I have been an US tech for almost 25 years and have done plenty of renal artery exams on native kidneys, but never on a transplant. I have one coming in tomorrow and now with your help I feel confident in obtaining a good study. Thanks so much!!
LikeLike