

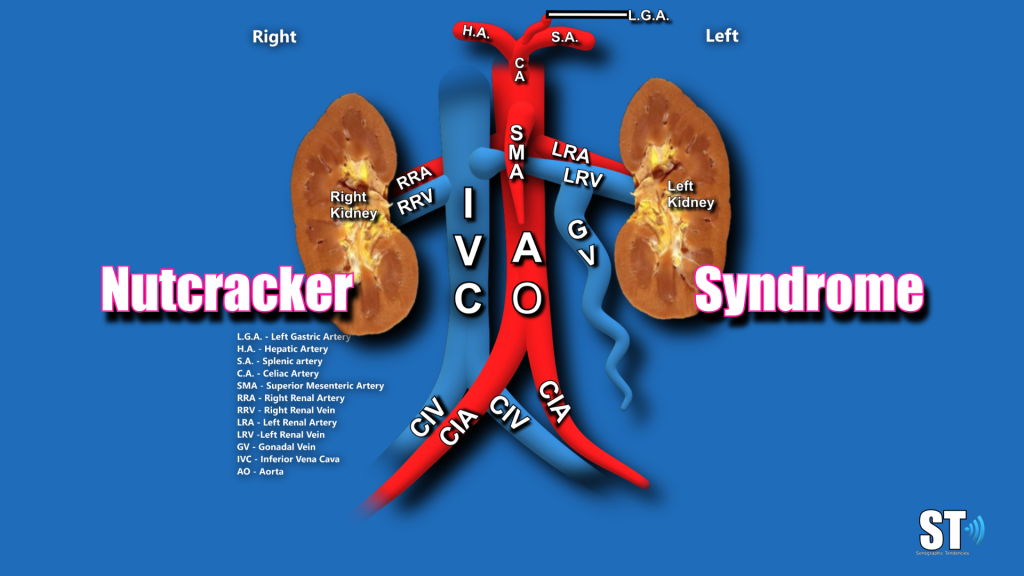
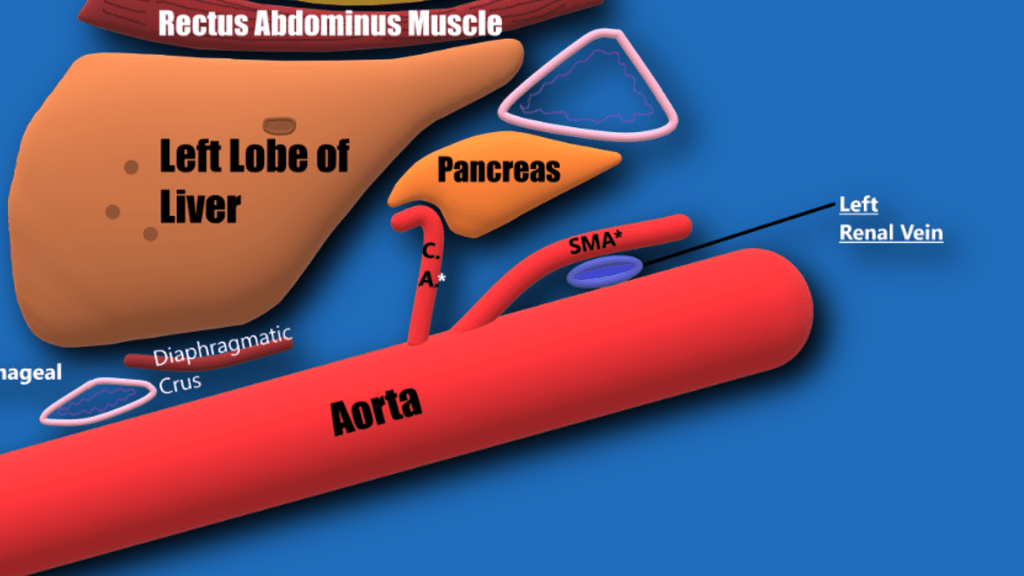
IntroductionNutcracker syndrome was first described in the literature by El-Sadr and Mina in 1950 [1]. It is considered a vascular compression disorder akin to May-Thurner syndrome (left iliac vein is compressed by the right iliac artery) and Thoracic outlet syndrome (compression of the vessel of the upper extremity)[2]. In normal anatomy the left renal vein courses between the Aorta and Superior Mesenteric Artery(SMA) (Diagram). If the descent of the SMA is too steep and/or the aorto-mesenteric angle too acute (normal angle is 38–65°) this could lead to left renal vein compression and Nutcracker syndrome/phenomenon. The difference between Nutcracker syndrome and phenomenon is the presence of symptoms in the syndrome and the lack of them in the phenomenon. Thus is the purpose of this review to illustrate a case of Nutcracker phenomenon in a patient with no symptoms or laboratory findings. The most common type of compression seen in Nutcracker Phenomenon/Syndrome is left renal vein compressed between the aorta and superior mesenteric artery also known as “anterior nutcracker”. A posterior type of compression may be seen with the retroaortic left renal vein anatomical variant, with the compression between the aorta and vertebrae, it is rare.
Symptoms
- Hematuria (Macro/microscopic rupture of thin-walled varices, due to elevated venous pressure, into the collecting system)
- Proteinuria
- Left-sided flank/lower abdominal/pelvic pain
- Varicose veins
- Urinary frequency
- Left-sided varicocele (or pelvic varices)


Types
There are 2 types of Nutcracker compression
Classic or anterior type which is compression of the LRV between the Aorta and SMA
Posterior which is when the anatomical variant of retrocaval LRV (when the left renal vein goes posterior to the IVC) and is compressed between the IVC and vertebrae.
Ultrasound
Sonography is an important tool in evaluating kidneys for size, shape, location and echogenicity. Compared to other modalities it is the most cost effective. It is very adept at discovering lesions and various causes of hematuria i.e. nephrolithiasis, tumors etc.. With ultrasound we evaluate the kidneys and the urinary bladder and other retroperitoneal structures. With color doppler you can interrogate the aorta, ivc, renal arteries and veins which is of paramount importance in discovering renal vein compression, renal artery stenosis and renal vein thrombosis to name a few.
Sonographically there will be an acute aortomesenteric angle <36°
Measure the compression ratio = P-C/C (P = pre-compressed vein C= compressed vein, CR >2.25 is indicative of NCS). Image the vessels in sagittal and transverse

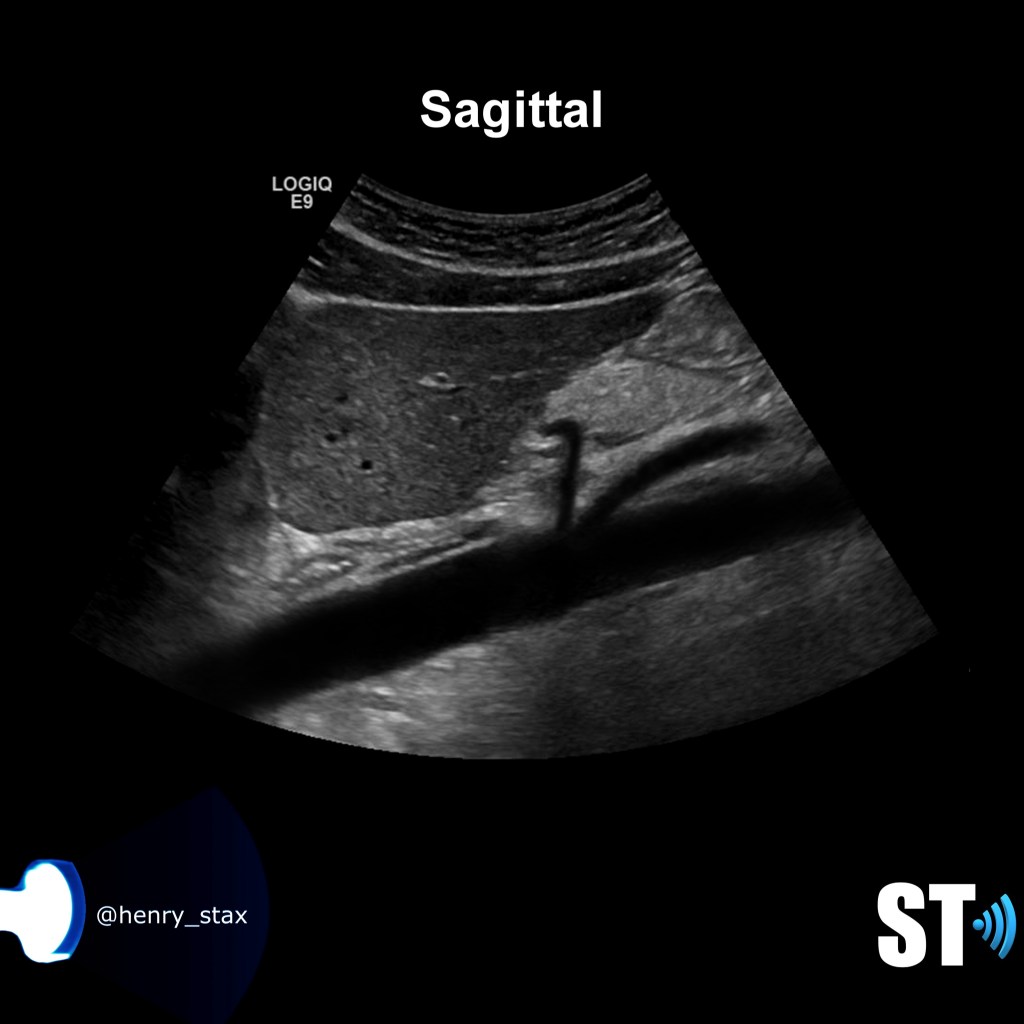


Nutcracker Phenomenon (asymptomatic patient)

Conclusion
Nutcracker syndrome continues to be an underreported disease. Ultrasound is quite effective in discovering this condition but it is also of great importance that sonographers are trained and made aware of this condition. It is quite possible that a small percentage of patients with left flank pain and hematuria without a known cause can have an undiagnosed nutcracker syndrome. As such our institution routinely looks for this condition when renal dopplers are performed especially with an ordering diagnosis of hematuria.

Hopped on from insta; thanks for the info. Would you mind posting how to measure the angle? For the nutcracker phenomenon or syndrome diagnosis is this a must for this protocol?
LikeLike
Thanks sooo much the pictures and video were excellent!!
LikeLike
How to measure the angle.?. . Please inform.
Thanks.
LikeLike
Thanks for your info. It is helpful..
LikeLike